TPIAT: A Way Forward for Chronic Pancreatitis
TPIAT: A Way Forward for Chronic Pancreatitis https://pediatricsnationwide.org/wp-content/uploads/2022/09/Fall-22-Cover-Flattened-HEADER-FOR-WEB-1024x500.jpg 1024 500 Katie Brind'Amour, PhD, MS, CHES https://pediatricsnationwide.org/wp-content/uploads/2021/03/Katie-B-portrait.gif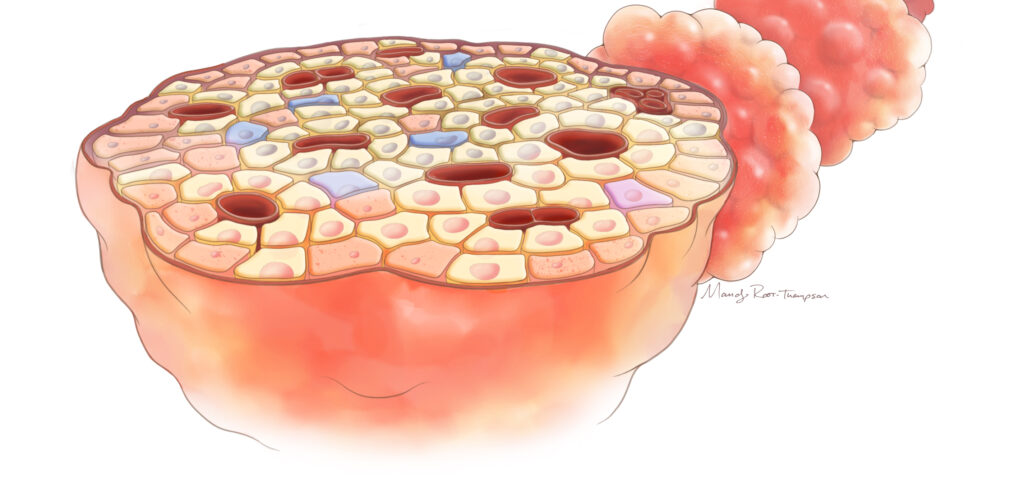
Nationwide Children’s Hospital has assembled a veritable “dream team” of pancreatitis and pediatric transplant surgery experts to offer what they hope will become the world’s preeminent pediatric center for complex pancreatic care.
Imagine your child suffering from a sudden, debilitating episode of abdominal pain. No obvious cause, no cure, just pain so severe it requires hospitalization for days — even weeks. Your child suddenly goes from an active, healthy kid to one who can’t tolerate a single bite of food.
This nightmare, acute pancreatitis, affects about 1 in every 10,000 U.S. children per year. The condition used to be considered a disease of adulthood, tied to alcohol use, smoking, gallstones, high cholesterol and certain medications. But as diagnosis and data collection improved among children, clinicians have documented an increasing incidence of acute pancreatitis almost matching that in adults.
Their kids aren’t thriving, they’re not growing, they’re having persistent pain. They have tried everything, without success. For many families, this is almost a hopeless situation — they can’t find the appropriate answers for their kids. — Oluyinka Olutoye, MD, PhD, surgeon-in-chief at Nationwide Children’s Hospital
Now, imagine that your child is one of the 15-35% who have a second attack. Your child is hospitalized again, recovers again. Only to fall prey to another and then another episode of pancreatitis — now considered acute recurrent pancreatitis. Eventually, damage to your child’s pancreas accumulates, and chronic pancreatitis (CP) develops. The pain is nearly constant and interferes with school, sports and social activities.
Your child can no longer lead a normal life, even with the use of round-the-clock pain medication.
“If you talk with families, you learn that this is such a frustrating, debilitating condition,” says Oluyinka Olutoye, MD, PhD, surgeon-in-chief at Nationwide Children’s Hospital. “Their kids aren’t thriving, they’re not growing, they’re having persistent pain. They have tried everything, without success. For many families, this is almost a hopeless situation — they can’t find the appropriate answers for their kids.”
This tragedy is a reality for almost 6 in every 100,000 children in the United States, about two-thirds of whom require frequent opioid use for pain management. Pancreatic function may be lost over time as the organ fights inflammation, blocked pancreatic ducts, scarring or other damage, resulting in the need for insulin or digestive enzyme medications in many children. Even with the best supportive care, about half of all patients with CP don’t achieve adequate pain relief from medication or endoscopic procedures and eventually require surgical intervention.
CP Surgery: What are the Options?
Conventional pancreatic operations aim to relieve pain by correcting an anatomical or morphological problem such as a blocked duct, poor drainage or an inflammatory mass in the head of the pancreas. Options include the modified Puestow procedure (also called a longitudinal pancreaticojejunostomy), the Whipple (pancreaticoduodenectomy), and duodenum-preserving pancreatic head resections (the Beger, Berne and Frey procedures).
Selecting an operation has a lot to do with what we think the underlying cause of a child’s pain is. Ductal strictures or pancreatic lesions may be amenable to focused surgical approaches, but for hereditary pancreatitis and those with truly unrelenting pain, a lot of the conventional procedures haven’t been hugely effective in the pediatric population. – A. Jay Freeman, MD, medical director of Pancreas Care at Nationwide Children’s Hospital
Unfortunately, it’s not as simple as choosing one from among many good options. Most of these surgical procedures carry significant risks, and as many as half of those who undergo these conventional operations do not enjoy lasting pain relief. They also still face an elevated risk of diabetes, opioid dependence and pancreatic cancer.
“We think of surgery as a last resort, only after medical and endoscopic management have failed, and it’s often not a miracle cure,” says A. Jay Freeman, MD, MS, medical director of Pancreas Care at Nationwide Children’s and a recent recruit from his role as director of the Advanced Pancreatic Care Program at Children’s Healthcare of Atlanta. “Selecting an operation has a lot to do with what we think the underlying cause of a child’s pain is. Ductal strictures or pancreatic lesions may be amenable to focused surgical approaches, but for hereditary pancreatitis and those with truly unrelenting pain, a lot of the conventional procedures haven’t been hugely effective in the pediatric population.”
This has increased the importance of imaging and interventional endoscopy in pre-surgical pancreatic care.
“What we want to do through a cohesive, multidisciplinary team is gather as much information as possible so that we have the best surgical outcomes — before we ever even operate,” says Muhammad Khan, MD, FASGE, director of advanced interventional endoscopy services at Nationwide Children’s. He is an expert in advanced abdominal imaging and endoscopic therapies and is fellowship-trained in endoscopic retrograde cholangiopancreatography and endoscopic ultrasound.
“That requires a robust genetic and molecular evaluation of patients, endocrinologic function evaluations and, of course, imaging and endoscopy is critical for virtually every child who progresses to surgery,” says Dr. Khan.
Procedures that preserve healthy tissue and provide resection and/or drainage approaches are considered appropriate options for some children with debilitating CP. Depending on the operation and underlying risk factors, as many as 85% of patients (based on adult data) who undergo duodenum-preserving pancreatic head resections experience meaningful reductions in pain. And nearly 3 in every 4 patients undergoing surgery found it helpful, according to a cohort of children in the INternational Study Group of Pediatric Pancreatitis: In search for a cuRE (INSPPIRE) project.
“Until we find a cure, there is certainly a place for these types of operations in the care of children with chronic pancreatitis,” says Jaimie Nathan, MD, FACS, chief of Pediatric Abdominal Transplant and Hepatopancreatobiliary Surgery at Nationwide Children’s and the most experienced board-certified pediatric surgeon in the country specializing in pancreatitis. “The key is making sure that the right operation is selected for the right patient, at the right time in the treatment continuum.”
At most hospitals, however, care often follows a predictable trajectory, ending with conventional drainage and/or resection procedures. If those don’t work, patients are simply in pain and out of luck.
Thankfully, a position statement released this year by the Pancreas Committee of NASPGHAN (North American Society for Pediatric Gastroenterology, Hepatology and Nutrition), with Dr. Nathan as its lead author, now offers sophisticated guidance for the consideration of pancreas anatomy and morphology in the selection of a surgical procedure for pediatric CP.


The guidelines strongly urge clinicians to consider genetic risk factors, which may predispose children to more complicated disease, poorer surgical outcomes and medication-resistant pain. Once hereditary status is known, making the best decision requires advanced imaging and in-depth, multidisciplinary discussion of the child’s pancreas health, disease physiology and probable outcomes.
In most cases, none of the conventional operations are a good fit for a child’s disease. It used to be that conventional procedures would be tried anyway. But in 1989, adult surgeons started incorporating a more extensive procedure into their care of children with CP: the total pancreatectomy with islet autotransplantation, or TPIAT.
Getting to Know TPIAT
TPIAT was first developed for the treatment of debilitating pancreatitis in adults in 1977. The procedure involves complete removal of the pancreas together with the isolation of the pancreas’ insulin producing islets, which are then introduced into the patient’s liver in the hope that they will continue their valuable work in a new home.
If you use a non-TPIAT operation on a patient that had high likelihood of failing, you’ve burned bridges. — Jaimie Nathan, MD, chief of Pediatric Abdominal Transplant and Hepatopancreatobiliary Surgery at Nationwide Children’s Hospital
As the pediatric gastroenterology community became more aware of pancreatitis in children, the procedure gradually migrated into the list of surgical options for young patients at some institutions. The results were remarkable.
In an Annals of Surgery study of 75 pediatric patients, 90% experienced improvements in pain and had stopped taking opioids 2 years postoperatively. Improvements in quality of life were equally robust, with almost universal freedom from CP-related school absences and significant improvements in all domains on a standard quality of life tool. Forty-one percent achieved insulin independence, with high durability of response as of 10 years post-surgery.
However, very few surgeons in the country have extensive experience performing the procedure in children, and those that do often get patient referrals only after multiple other operations have failed.
“If they don’t have the anatomic features to consider non-TPIAT options, all you can offer is TPIAT,” says Dr. Nathan, who has cared for this population for more than 10 years and performed nearly 100 TPIATs since 2015.
A high percentage of children with acute recurrent and chronic pancreatitis do not have a dilated main pancreatic duct or an inflammatory head mass, which rules out the utility of surgical drainage procedures and partial resections, respectively.
“Even in children with a dilated duct or pancreatic head mass, if they have an underlying genetic risk factor, it’s unlikely that an operation other than TPIAT is actually still the optimal approach,” Dr. Nathan says. Pancreatic inflammation, organ fibrosis, partial resections and drainage operations reduce the number of islets remaining in the pancreas. Delaying the use of TPIAT until after other operations have been attempted and failed may not be the best tactic.
“If you use a non-TPIAT operation on a patient that had high likelihood of failing, you’ve burned bridges,” says Dr. Nathan. “They often muddle through, not relieved of their pain, staying on opioids or coping with chronic pain longer before they get to a salvage TPIAT, and in the interim they may develop central sensitization. At that point, the patient has also faced a much longer duration of disease, and you’ve missed the opportunity to maximize islet isolation yield and the potential for coming off exogenous insulin.”
Despite complete resection, up to 1 in 10 patients may continue to experience pain after TPIAT, likely due to central sensitization (much like phantom limb pain after an amputation). And since the entire pancreas is removed, children also require pancreatic enzyme replacement therapy (PERT) for life. General complication rates are low, though — comparable to or better than conventional operations when TPIAT is done by an experienced surgeon.
As research continues, the goal is to refine the ideal point of intervention and the best population for the procedure. Some data support the use of TPIAT earlier in the treatment continuum than initially anticipated because of better pain relief (100%) and insulin independence rates (64%) among 3-to-8-year-olds compared to older children. This may reflect the fact that islet health is likely to be better earlier in the disease course — a critical factor for diabetes prevention — and sensitization is less likely to have developed.
The Prospective Observational Cohort Study of TPIAT (the POST Study), which Dr. Nathan led as the site principal investigator at his prior institution and is now in the data analysis phase, hopes to determine whether patients with central sensitization, as assessed by quantitative sensory testing, have poorer long-term TPIAT outcomes. Additional research efforts at Nationwide Children’s aim to further evaluate and improve outcomes for TPIAT patients.
“Offering this advanced medical care and surgical service goes to the next level of achieving best outcomes for an important subgroup of patients who can’t have their needs met by other means,” says Dr. Olutoye, who helped orchestrate the CP “dream team” recruitment and program development plans together with the medical leadership in gastroenterology at Nationwide Children’s. “Also having the ability to isolate the islets and advance autotransplantation science right here, though, is the key to making this truly unique.”
The Science of Islet Autotransplantation
The pancreas contains clusters of cells called islets, which collectively manage the body’s blood glucose levels by secreting insulin. They make up only about 2% of pancreatic cells and depend on a network of vascular connections to monitor blood sugar and respond accordingly.
For TPIAT, the islets are isolated from the removed pancreas and the non-islet tissue via an enzyme digestion by a team of scientists in a Good Manufacturing Process (GMP) clean room. The goal is to maximize the number of healthy islets that can be re-implanted into the patient to prevent diabetes. The islets are then introduced into the liver via the portal vein. Upon arrival, the islets must re-establish a blood supply, which usually takes several weeks, before they can adjust blood glucose levels via insulin production.
“My research career has focused on manufacturing and optimizing pancreatic islet cell products for clinical transplantation studies, and specifically improving islet yield from every processed pancreas,” says Balamurugan Appakalai, PhD, director of the Pancreatic Islet Cell Isolation Program and a principal investigator in the Center for Clinical and Translational Research in the Abigail Wexner Research Institute at Nationwide Children’s. “We have established advanced islet manufacturing protocols for clinical islet autotransplantation.”
Total Pancreatectomy with Islet Autotransplantation (TPIAT): Inside Dr. Balamurugan Appakalai's Lab
Dr. Appakalai is among the world’s most experienced in processing human pancreases for clinical islet autotransplantation and allotransplantation. He has processed more than 1,500 pancreases, which have been utilized for clinical auto- and allotransplantation and for islet biology research initiatives. His research has been dedicated to methods to preserve and improve blood circulation to isolated islets after transplantation.
To achieve consistent success in clinical outcomes, an islet isolation team must learn to recognize key variables of a pancreas, such as fibrosis and patient age. They must also understand the principles of the isolation procedure well enough to adapt it for each individual organ. Dr. Appakalai and his team are working to improve the survival of transplanted islets after separation from the native pancreas, focusing on providing blood supply to transplanted islets immediately after infusion into the liver. His team also works with stem cell approaches to generate insulin-producing cells in the lab.
“I am grateful that there is such a strong and growing clinical utility for my work,” says Dr. Appakalai, who has processed more than 1,500 pancreases. “And working with a collaborative, science-friendly team of endocrinologists, gastroenterologists, surgeons and radiologists will help us continue to improve the success of our science at the bedside and at the bench.”
The team’s on-site GMP islet facility is the only one of its kind at a pediatric hospital in the United States, and will also process pancreases for TPIAT performed at other institutions — providing the opportunity for the operation to be offered at centers that do not have a local islet isolation facility.
A Bright Future for CP Care
As research continues to confirm that pediatric TPIAT is safe and effective at providing lasting pain relief for children with advanced CP, this procedure is poised to offer a very promising alternative to conventional operations. Coupled with improvements in islet isolation and transplantation technology, it appears likely that TPIAT will soon become more commonplace in the surgical management of pediatric CP.
“TPIAT isn’t a service that you dabble in,” says Dr. Olutoye. “You have to commit as an institution to recruit the experts in the field, and to not just provide the service but be poised to advance the field with the level of medical care, imaging resources, surgical expertise, pain management, and the scientific and clinical research efforts that these patients deserve. This is a crucial need for these families, so if we can help them achieve best outcomes, we are invested in it 100%.”
The growing team and pancreatitis-related offerings have already made Nationwide Children’s the epicenter for advanced treatment of pediatric CP, TPIAT and islet transplantation research. But the capabilities of the “dream team” have important benefits for other patients, as well, both in terms of broadened research capacity and expanded clinical care offerings.
“The growth of the pancreas care program means that we can offer comprehensive care and screening after acute pancreatitis episodes to identify important complications early,” says Cheryl Gariepy, associate division chief of Gastroenterology, Hepatology and Nutrition at Nationwide Children’s. She is a long-time principal investigator for INSPPIRE and a key member in helping Nationwide Children’s gain recognition as a National Pancreas Foundation Center of Excellence for both clinical care and academic research. “It also means that a team of providers with internationally recognized expertise will be able to offer all of the most advanced services and procedures to children with pancreatic disease in one place.”
The team’s surgeons and clinicians will also collaborate on all solid organ transplants, as well as clinical care and outcomes for children with other pancreatic, liver, biliary tract and gastrointestinal disorders. Dr. Khan is also busy expanding the interventional endoscopy component of the program with novel treatments for the entire gastroenterology department’s patient population, carried out in a custom-built interventional endoscopy suite.
“We have great support to build a leading global program with an interdisciplinary pancreatic pain clinic, state-of-the-art imaging, the nation’s most robust surgical offerings and a collaborative team of experts that can offer a truly holistic approach to pain management and pancreatic care,” says Dr. Freeman. “That makes a big difference in a patient’s experience when they seek out treatment for a rare and challenging disease, and I am excited to be part of this.”
This feature was published in the Fall/Winter 2022 issue. Download the full issue.
References:
- Chinnakotla S, Bellin MD, Schwarzenberg SJ, Radosevich DM, Cook M, Dunn TB, Beilman GJ, Freeman ML, Balamurugan AN, Wilhelm J, Bland B, Jimenez-Vega JM, Hering BJ, Vickers SM, Pruett TL, Sutherland DE. Total pancreatectomy and islet autotransplantation in children for chronic pancreatitis: indication, surgical techniques, postoperative management, and long-term outcomes. Annals of Surgery. 2014;260(1):56-64.
- INSPPIRE. “About our research: INSPPIRED to find a cure for pediatric pancreatitis.” Stead Family Department of Pediatrics, Carver College of Medicine, University of Iowa. Accessed online 28 June 2022.
- Nathan JD, Ellery K, Balakrishnan K, Bhatt H, Ganoza A, Husain SZ, Kumar R, Morinville VD, Quiros JA, Schwarzenberg SJ, Sellers ZM, Uc A, Abu-El-Haija M. The role of surgical management in chronic pancreatitis in children: a position paper from the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition Pancreas Committee. Journal of Pediatric Gastroenterology and Nutrition. 2022 May 1;74(5):706-719.
- Perito ER, Palermo TM, Pohl JF, Mascarenhas M, Abu-El-Haija M, Barth B, Bellin MD, Fishman DS, Freedman S, Gariepy C, Giefer M, Gonska T, Heyman MB, Himes RW, Husain SZ, Lin T, Liu Q, Maqbool A, McFerron B, Morinville VD, Nathan JD, Ooi CY, Rhee S, Schwarzenberg SJ, Shah U, Troendle DM, Werlin S, Wilschanski M, Zheng Y, Zimmerman MB, Lowe M, Uc A. Factors associated with frequent opioid use in children with acute recurrent and chronic pancreatitis. Journal of Pediatric Gastroenterology and Nutrition. 2020 Jan;70(1):106-114.
Image credits: Nationwide Children’s
About the author

Katherine (Katie) Brind’Amour is a freelance medical and health science writer based in Pennsylvania. She has written about nearly every therapeutic area for patients, doctors and the general public. Dr. Brind’Amour specializes in health literacy and patient education. She completed her BS and MS degrees in Biology at Arizona State University and her PhD in Health Services Management and Policy at The Ohio State University. She is a Certified Health Education Specialist and is interested in health promotion via health programs and the communication of medical information.
- Katie Brind'Amour, PhD, MS, CHEShttps://pediatricsnationwide.org/author/katie-brindamour-phd-ms-ches/

- Katie Brind'Amour, PhD, MS, CHEShttps://pediatricsnationwide.org/author/katie-brindamour-phd-ms-ches/
- Katie Brind'Amour, PhD, MS, CHEShttps://pediatricsnationwide.org/author/katie-brindamour-phd-ms-ches/
- Katie Brind'Amour, PhD, MS, CHEShttps://pediatricsnationwide.org/author/katie-brindamour-phd-ms-ches/