
Single Ventricle, Many Research Angles
Single Ventricle, Many Research Angles https://pediatricsnationwide.org/wp-content/uploads/2025/03/for-web-Insight-Right_FINAL_Cropped-1-pdf-1024x658.jpg 1024 658 Katie Brind'Amour, PhD, MS, CHES https://pediatricsnationwide.org/wp-content/uploads/2021/03/Katie-B-portrait.gif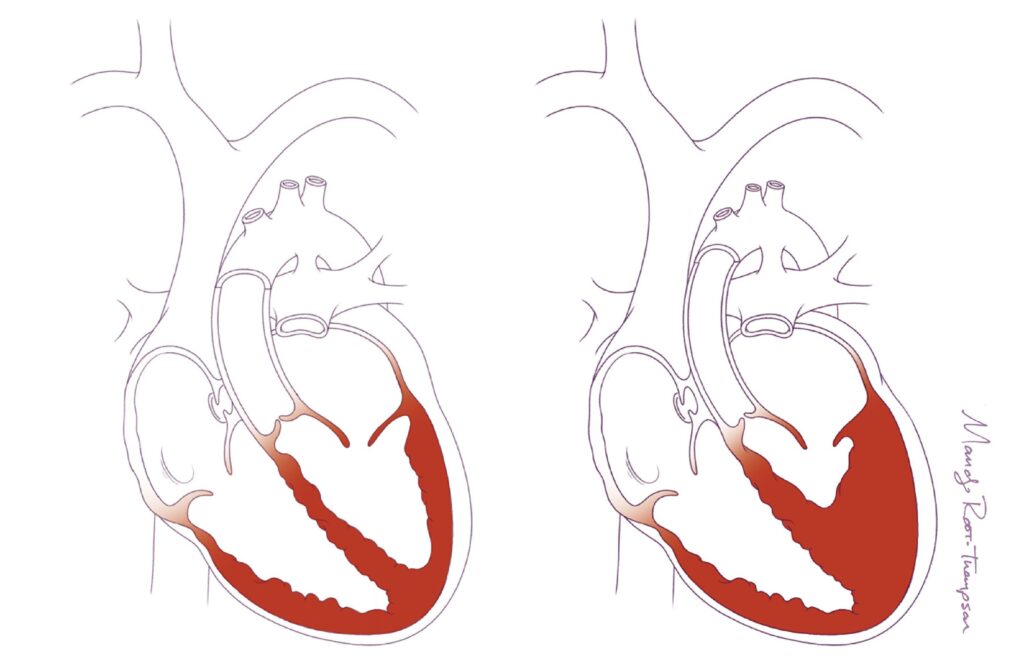
An overview of the people and projects behind one of the world’s most robust single-ventricle heart disease research hubs.
In the field of single-ventricle heart disease (SVHD), there are more questions than answers.
What causes the heart to form with only one ventricle? At what point in fetal development might we intervene to improve its development or function? Which children have the greatest risk for poor outcomes? Can novel surgical approaches normalize a child’s expected quality and quantity of life? What promise might medical or gene therapies hold? Can SVHD be cured altogether?
Advances in many other types of congenital heart disease (CHD) have dramatically improved survival for many patients — so much so that it has given rise to a new board-certified field of medical practice, adult CHD. But improvements have been slower in SVHD. It is fatal by the age of 10 in nearly half of children born with hypoplastic left heart syndrome (HLHS), and survival in children with other types of SVHD is not much better. Those who do survive often have major impacts on quality of life, such as limitations on physical activity, increased neurodevelopmental risks and poorer psychosocial health.
While CHD affects as many as 1% of babies born in the United States, the different forms of SVHD together affect about 1,000 U.S. babies each year.
To complicate matters, SVHD has many possible variations, requiring patient-specific approaches, early intervention and numerous procedures to save the child’s life. The Norwood and Glenn surgical approaches first provided life-saving advances for babies with hypoplastic right and left heart syndromes. However, until the development of a surgical procedure called the Fontan — in which surgeons bypass the heart to deliver oxygen-poor blood straight to the lungs without passing through the heart — babies with SVHD remained cyanotic. Even with the advent of the Fontan, long-term outcomes leave much to be desired.
“To an extent, the increasing interest in SVHD is driven by where we are in pediatric cardiology and cardiothoracic surgery,” explains Vidu Garg, MD, director of the Center for Cardiovascular Research and co-director of The Heart Center at Nationwide Children’s, and a practicing cardiologist. “With some heart defects, surgical closure of a hole is all that is needed and we anticipate that these patients will live a normal, healthy life. But with SVHD, there is still a huge need to improve outcomes. We have a lot to learn.”
Tissue Talent
Researchers have flocked to Nationwide Children’s to join in a growing, diverse community of scientists and clinicians dedicated to improving the outlook for patients with SVHD.
One of the latest arrivals is Daisuke Onohara, MD, PhD, principal investigator in the Center for Regenerative Medicine at the Abigail Wexner Research Institute (AWRI), who recently developed the first successful large animal model for SVHD in lambs.
“There are several good small animal models for HLHS, but there are still many limitations to understanding this disease, which is multigenic and heterogenous,” says Dr. Onohara. His model, developed during his time at Emory University School of Medicine, introduces a balloon catheter at 120 days’ gestation in fetal lambs to block the mitral valve, after which the reduced flow of blood through the left ventricle induces HLHS.
“That [induction of single-ventricle disease] in a large animal model is powerful on so many different levels,” says Christopher Breuer, MD, director of the Center for Regenerative Medicine at AWRI. “It’s a model for testing new therapies, it will help us understand how SVHD forms and it will give us insights into better therapeutics that could be curative instead of just palliative.”
Dr. Breuer has already initiated a collaboration with Dr. Onohara to study fetal heart valve replacement using tissue-engineered valves.
“There is a theory in the field of ‘no flow, no grow,’ meaning any sort of anomaly that blocks or reduces flow through the ventricle can induce hypoplasia and the lack of ventricle formation in the fetus,” says Dr. Breuer.
Some interventional cardiologists and perinatologists have conducted fetal valvuloplasty for the past decade or so, which involves opening the valve via angioplasty during the third trimester. Some of those children go from having a single ventricle back to normal biventricular anatomy. Unfortunately, the heart valve remains abnormal and typically requires replacement during the newborn or early childhood period.
Dr. Breuer’s goal is to replace the valve in utero with a tissue-engineered (TE) valve that will function normally and grow with the child — offering a chance at a cure.
Dr. Breuer and his long-time research partner, Toshiharu Shinoka, MD, PhD, co-director of the Tissue Engineering Program at Nationwide Children’s and a principal investigator in the Center for Regenerative Medicine at AWRI, have been developing, improving and studying TE scaffolds for more than 20 years. The idea of TE valves utilizes techniques already supported by a growing body of clinical research on their tissue-engineered vascular graft (TEVG), including the first-ever FDA-approved TEVG trial in children. The scaffold offers a biodegradable replacement vessel seeded with the patient’s own cells for patients with SVHD undergoing the Fontan procedure.
Current synthetic conduits used in the Fontan procedure do not grow with the patient and may end up with complications such as thromboembolic events and stenosis, which may eventually require reintervention to place a stent or even another open-heart surgery to replace the graft. TEVG scaffolds, however, enable the patient’s body to grow native blood vessel tissue that is vasoreactive and compliant and grows with the patient. Findings to date suggest they could eliminate the need for new grafts as patients age.

That [induction of single-ventricle disease] in a large animal model is powerful on so many different levels. It’s a model for testing new therapies, it will help us understand how SVHD forms and it will give us insights into better therapeutics that could be curative instead of
just palliative.”— Christopher Breuer, MD, director of the Center for Regenerative Medicine at Nationwide Children’s
Hybrid Hearts
TEVG is just one research vein targeting improved surgical outcomes for patients with SVHD. Cardiac surgeons in The Heart Center at Nationwide Children’s constantly re-evaluate surgical management of HLHS and borderline HLHS. Having spearheaded the development and adoption of the hybrid surgical approach for HLHS, they lead the nation in the number of these operations they perform.
“A few decades ago, it was becoming very clear that improvements with the traditional approach to single ventricle surgery had plateaued, and people needed to start thinking differently, in a new platform,” says Mark Galantowicz, MD, chief of cardiothoracic surgery and co-director of The Heart Center at Nationwide Children’s. “That led to the hybrid approach, which has become a paradigm-shifting tool in many centers around the world.”
“A few decades ago, it was becoming very clear that improvements with the traditional approach to single-ventricle surgery had plateaued and people needed to start thinking differently, in a new platform. That led to the hybrid approach, which has become a paradigm-shifting tool in many centers around the world.”
— Mark Galantowicz, MD, chief of cardiothoracic surgery and co-director of The Heart Center at Nationwide Children’s
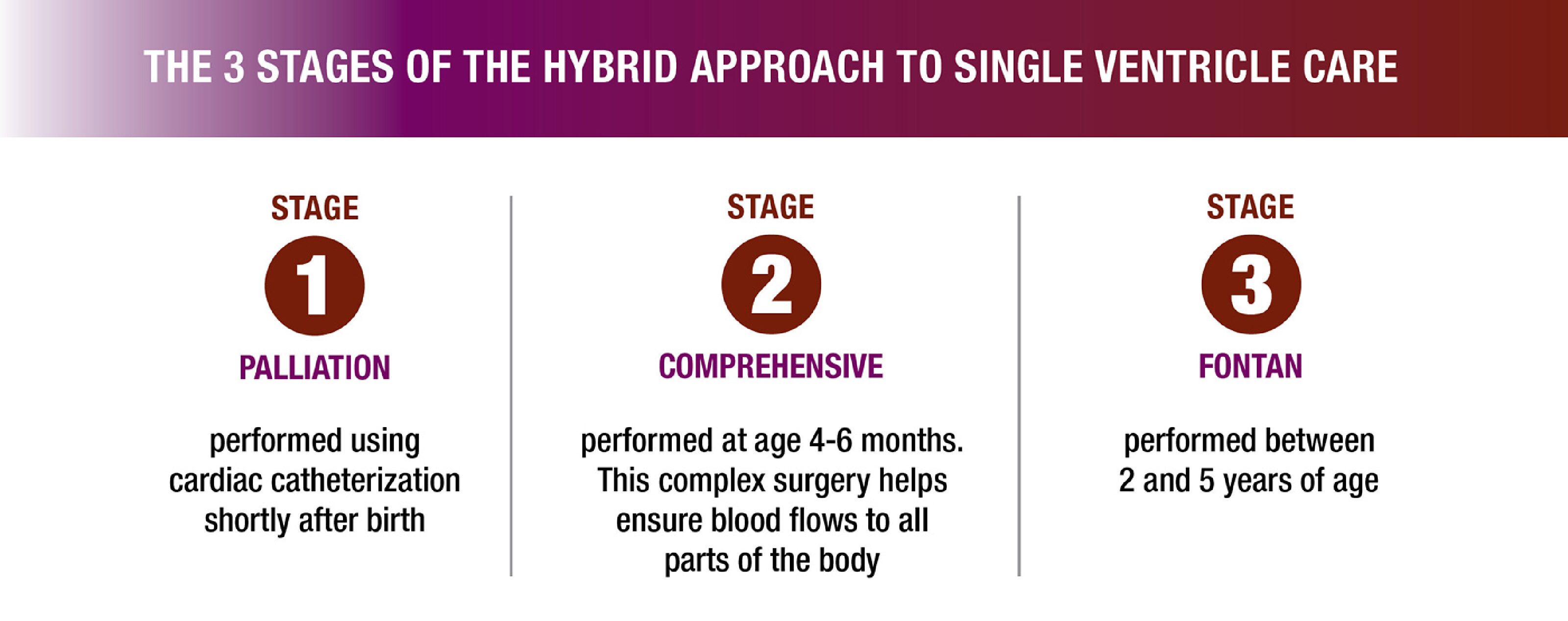
The hybrid approach for SVHD minimizes the invasiveness of intervention during the neonatal period, protecting the baby’s brain and other vital organs by delaying the more complex, open-heart procedures until they have grown in strength and size. The fact that the initial treatment is easier than the prior standard management of HLHS patients also means that children born at institutions with fewer resources for complex surgeries can now survive; local surgeons can perform the hybrid stage 1 procedure and then transfer the child to a more suitable facility for open-heart surgery when needed.
With more than 20 years of experience in the procedure, hybrid experts at Nationwide Children’s have set their sights on the next steps in transforming surgical success for patients with SVHD: understanding variation in the surgical technique’s use and outcomes, clarifying best practices, promoting the adoption of hybrid approach guidelines, designating Centers of Excellence and further refining the optimal surgical approach for different single-ventricle anomalies.
“Invariably, these patients are at high risk, and they suffer from this condition for their whole lives,” says Can Yerebakan, MD, PhD, associate chief of the Department of Cardiothoracic Surgery and principal investigator in the Center for Cardiovascular Research — and another recent addition to The Heart Center at Nationwide Children’s. “If we can have fetal genetic, surgical or combined interventions that can prevent single-ventricle disease from developing, it could be an important way to influence the fate of these patients. Even if we just lessen its severity to a borderline disease, we have effective surgical and interventional approaches for that, and we can really help those patients.”
Dr. Yerebakan specializes in the hybrid approach for HLHS and borderline left ventricle disease, in which the left heart is partially underdeveloped but not totally nonfunctional. These patients may benefit from customized adaptations to the hybrid approach to try to stimulate ventricle function and growth rather than undergo primary surgical transition to single-ventricle anatomy. The addition of his expertise further cements the Nationwide Children’s team as the most experienced hybrid surgeons in the country.
“Unfortunately, the Fontan will always be a palliative operation and not curative, and TEVG may improve quality of life and longevity but it also can never fully fix the problem,” says Dr. Breuer. “At the end of the day, they still have a single ventricle and abnormal hemodynamics.”
That’s why numerous teams at Nationwide Children’s study the genomic, epigenetic and pathophysiologic aspects of SVHD, using everything from chicks to CRISPR — including Dr. Yerebakan’s burgeoning laboratory endeavors at Nationwide Children’s, which involve collaboration with Dr. Onohara to identify the optimal time to intervene during fetal development to reverse HLHS. Dr. Yerebakan also studies SVHD development in a chick embryo model to better understand potential biological causes.
Additional endeavors now underway at Nationwide Children’s include the use of human induced pluripotent stem cells (iPSCs) to study a host of different aspects of SVHD.

Donations and Diagnostics
Human iPSCs from patients with SVHD are easily available to researchers both within and external to Nationwide Children’s, courtesy of the research endeavors of Mingtao Zhao, DVM, PhD, principal investigator in the Center for Cardiovascular Research at AWRI, who has recruited more than 200 patients with SVHD and generated more than 70 iPSC lines from their donated blood samples.
While the cells can be used to grow any type of tissue for study — including different heart cell types or brain or liver cells, all of which could reveal valuable information about the impact of SVHD genotypes on different organs— Dr. Zhao uses them for three projects of his own.
The first project, with proof of principle already published in Circulation Research, uses cell-free RNA circulating in maternal blood to diagnose SVHD in the fetus. Predicting SVHD early in pregnancy with a simple test could help identify babies earlier who might not otherwise have access to the advanced ultrasound services used to study these defects. Earlier diagnosis means more time to plan appropriate interventions, get the right surgeons identified and — once more fetal therapies are available — a better chance at a cure.
Unfortunately, numbers are a challenge. Because of the rarity of the disease, Dr. Zhao must recruit enough participants to validate his panel in a larger cohort before he seeks approval for the diagnostic test from the U.S. Food and Drug Administration. HLHS affects about 1 in every 4,000 newborns. HRHS affects just 1 in 10,000.
“It is challenging, but we will make every effort to realize this diagnostic as soon as we can,” says Dr. Zhao. He is also working to determine whether the cell-free RNA in the mother’s blood samples can distinguish between different types of SVHD.
His second project involves the study of HRHS using patient-specific iPSCs. Initial findings were also published in Circulation, suggesting HRHS may be caused by the abnormal development of early heart progenitors that give rise to major cell types in the right side of the heart.
Dr. Zhao’s other main endeavor involves CRISPR/Cas-9 genome editing, also using the SVHD iPSC lines he established. For this work, he collaborates with colleagues such as Dr. Garg, using CRISPR genome editing to engineer and study the impact of a transcriptional regulator called NOTCH1, known to be involved in many types of CHD. By deleting it in normal iPSC lines, he can study how its absence impacts cardiomyocyte differentiation and proliferation, which he has published in Circulation Research. In SVHD iPSC lines, he wants to see how CRISPR/Cas9-based genomic correction of a NOTCH1 mutation affects the phenotype.
“The genetics of SVHD are very complex,” Dr. Zhao explains. “NOTCH1 is a contributor, but there are many others — a mutation may collaborate with a few or even a dozen genes to collectively contribute to a phenotype.”
Not Just NOTCH1
Dr. Garg has been on the NOTCH1 bandwagon since he first identified it in his studies of bicuspid aortic valve, a condition considered genetically related to HLHS. Since then, he has focused on developing mouse models using NOTCH1 as the entry point for studying phenotypes such as aortic valve disease and HLHS. In recent research, Dr. Garg’s model combining NOTCH1 and GATA5 mutations results in up to 90% of the mice having an abnormal aortic valve at birth.
“Interestingly, these mice can survive into adulthood, so we can follow them as the valve stenosis gets more severe,” says Dr. Garg.

Now we can try to understand why the valve is not forming properly, and also look for novel therapeutics to remodel the valve at birth or slow progression of the stenosis and see if this is an approach worth moving toward the clinic.”
— Vidu Garg, MD, director of the Center for Cardiovascular Research and co-director of The Heart Center at Nationwide Children’s
The idea behind his work is that by rescuing the aortic valve, blood flow through the valve and ventricle may enable the rest of the heart anatomy to develop properly. Dr. Garg’s goal dovetails with other efforts, including the work of Drs. Breuer and Onohara, to prevent SVHD by healing the valve in utero.
“Single ventricle disease is truly a syndrome, which makes understanding the genotype and phenotype and the molecular programs at play very important,” says Dr. Garg, who also investigates RBFOX2 variation as a key genetic driver of HLHS.
Together with a team of in-house cardiology, neonatology, medical genetics and genomics, data science and translational informatics experts, Dr. Garg is working to expand a genomic sequencing project called COURAGE for Kids from the neonatal intensive care unit to include patients in the cardiac ICU at Nationwide Children’s.
Supported by the Steve and Cindy Rasmussen Institute for Genomic Medicine at Nationwide Children’s, COURAGE for Kids should provide valuable insights into the presence and potential effects of various mutations in clinical outcomes.
Meanwhile, researchers in the Center for Cardiovascular Research continue to investigate other known genes of interest in CHD.

Puzzle Pieces
“We need to understand the fundamentals of the problem with more than just one approach before we can go further,” says Deqiang Li, MD, PhD, a principal investigator in the Center for Cardiovascular Research at AWRI who worked as a cardiac surgeon before dedicating his career to basic science.
In mouse models, HDAC3 mutations result in smaller, thinner, weaker or missing heart tissue — such as a hole in between heart chambers. Dr. Li and his team want to know why these phenotypes occur, including the pathways, cell communication and changes in function or roles of the gene over time during development.
Recent findings from his lab support a role for HDAC genes and related cellular cross-talk in myocardium development and muscle contractility, which could provide valuable context for SVHD research.
“Single-ventricle disease is a very complicated heart defect, and we all are working at one little piece of the puzzle that alone is nothing,” says Dr. Li. “But when you start to put the pieces together, you begin to see the big picture.”
The SVHD researchers at Nationwide Children’s credit their success to that big-picture vision and practical support from clinical and administrative leadership, which resulted in an advanced vivarium, state-of-the-art hybrid operating suites, genomics and CRISPR/Gene Editing Core resources, the iPSC Core and seed funding for numerous laboratories. The teams are now heavily funded by federal grants and advocacy organizations such as the American Heart Association and Additional Ventures.
“The field is moving forward faster than before, when funding was scarce and there were fewer parent and patient advocates driving interest,” says Dr. Zhao. “Now we’ve got people using the iPSC lines, small animal models, large animal models and even computational models to study SV disease.”
As the researchers make collective progress toward more answers for more patients, they are optimistic about improved therapies and even a cure for SVHD in the next few decades, be it from gene therapy, fetal intervention, TE valves, medical therapy or another approach.
“The overarching goal is improving the quality and quantity of life for these patients — and we’ve got a first-rate clinical program as well as a robust clinical research arm, animal research and benchtop scientists, and constant translational research. The stars have aligned here, and I feel that our institution is uniquely capable of expanding the horizon for patients with single-ventricle disease.”
This article appeared in the 2025 Spring/Summer issue. Download the issue here.
References
- Alonzo M, Xu Z, Yu Y, Ye S, Wang C, Wang J, McNutt M, Bering J, Ma Q, Texter K, Garg V, Zhao MT. Cell-free RNA signatures in maternal blood with fetal congenital heart disease. Circulation Research. 2024 Oct 25;135(10):1021-1024.
- Garg V, Muth AN, Ransom JF, Schluterman MK, Barnes R, King IN, Grossfeld PD, Srivastava D. Mutations in NOTCH1 cause aortic valve disease. Nature. 2005;437(7056):270-274.
- Hardisky D, Satija D, Texter K, Alvarado C, Galantowicz M, Carrillo SA. Efficiency at heart: navigating the hybrid single-ventricle pathway. Annals of Thoracic Surgery Short Reports. 2024;2(3):374-379.
- Jang J, Bentsen M, Kim YJ, Kim E, Garg V, Cai CL, Looso M, Li D. Endocardial HDAC3 is required for myocardial trabeculation. Nature Communications. 2024;15(1):4166.
- Miyachi H, Tara S, Nakayama H, Hama R, Sugiura T, Reinhardt JW, Yi T, Lee YU, Lee AY, Miyamoto S, Shoji T, Nakazawa Y, Breuer CK, Shinoka T. Transmural macrophage migration into an arterial bioresorbable vascular graft promotes inflammatory-mediated response and collagen deposition for vascular remodeling. Acta Biomaterials. 2024;183:146-156.
- Onohara D, Hagen M, Louey S, Giraud G, Jonker S, Padala M. Chronic in utero mitral inflow obstruction unloads left ventricular volume in a novel late gestation fetal lamb model. JTCVS Open. 2023;16:698-707.
- Turner ME, Blum KM, Watanabe T, Schwarz EL, Nabavinia M, Leland JT, Villarreal DJ, Schwartzman WE, Chou TH, Baker PB, Matsumura G, Krishnamurthy R, Yates AR, Hor KN, Humphrey JD, Marsden AL, Stacy MR, Shinoka T, Breuer CK. Tissue engineered vascular grafts are resistant to the
formation of dystrophic calcification. Nature Communications. 2024;15(1):2187. - Yasuhara J, Ueyama Y, Adamczak S, Cameron E, Garg V. Abstract 9782: Disruption of Notch1 and Gata5 in mice results in clinically relevant aortic valve disease. Circulation. 2021;144(S1).
- Ye S, Wang C, Xu Z, Lin H, Wan X, Yu Y, Adhicary S, Zhang JZ, Zhou Y, Liu C, Alonzo M, Bi J, Ramirez-Navarro A, Deschenes I, Ma Q, Garg V, Wu JC, Zhao MT. Impaired human cardiac cell development due to NOTCH1 deficiency. Circulation Research. 2023;132(2):187-204.
- Yu Y, Wang C, Ye S, Xu Z, Lin H, Texter K, Shukla V, Ghadiali S, Ma Q, Garg V, Zhao MT. Abnormal progenitor cell differentiation and cardiomyocyte proliferation in hypoplastic right heart syndrome. Circulation. 2024;149(11):888-891.
Image credits: Nationwide Children’s
About the author

Katherine (Katie) Brind’Amour is a freelance medical and health science writer based in Pennsylvania. She has written about nearly every therapeutic area for patients, doctors and the general public. Dr. Brind’Amour specializes in health literacy and patient education. She completed her BS and MS degrees in Biology at Arizona State University and her PhD in Health Services Management and Policy at The Ohio State University. She is a Certified Health Education Specialist and is interested in health promotion via health programs and the communication of medical information.
- Katie Brind'Amour, PhD, MS, CHEShttps://pediatricsnationwide.org/author/katie-brindamour-phd-ms-ches/

- Katie Brind'Amour, PhD, MS, CHEShttps://pediatricsnationwide.org/author/katie-brindamour-phd-ms-ches/
- Katie Brind'Amour, PhD, MS, CHEShttps://pediatricsnationwide.org/author/katie-brindamour-phd-ms-ches/
- Katie Brind'Amour, PhD, MS, CHEShttps://pediatricsnationwide.org/author/katie-brindamour-phd-ms-ches/


