
A New Therapeutic Era in Pediatric Functional and Motility Disorders
A New Therapeutic Era in Pediatric Functional and Motility Disorders https://pediatricsnationwide.org/wp-content/themes/corpus/images/empty/thumbnail.jpg 150 150 Katie Brind'Amour, PhD, MS, CHES https://pediatricsnationwide.org/wp-content/uploads/2021/03/Katie-B-portrait.gif20 years ago, treatment options were limited for children with functional gastrointestinal (GI) and motility disorders. Now, a growing list of drugs, behavioral and dietary care plans, and an advanced, forward-looking technique – neuromodulation – are transforming pediatric GI care.
Gastrointestinal (GI) disorders are notoriously difficult to diagnose. Virtually all functional and motility-related GI problems present with common symptoms: nausea, vomiting, abdominal pain, bloating, gas, diarrhea or constipation. Many patients wait months or even years for the right diagnosis, and even then, management of functional (often sensation-related) and motility (transit-related) disorders can be difficult. That’s why recent advancements in therapeutic options and outcomes research have been critical.
“In the late 90s and early 2000s there was really no treatment available to children with the most severe motility disorders,” says Carlo Di Lorenzo, MD, chief of the Division of Gastroenterology, Hepatology and Nutrition at Nationwide Children’s Hospital. “Now, we have medications, neuromodulation, surgical interventions, dietary treatment, and behavioral treatment – five different types of interventions that have the potential to help.”
Pharmaceutical treatments offer the most straightforward medical approach to some symptom relief, but some children require additional or alternate treatments, including surgery. Many emerging therapies, such as behavioral therapies and neuromodulation techniques, offer unique – often less invasive – strategies for reducing symptoms and even curing disease.
BOTOX® FOR KIDS
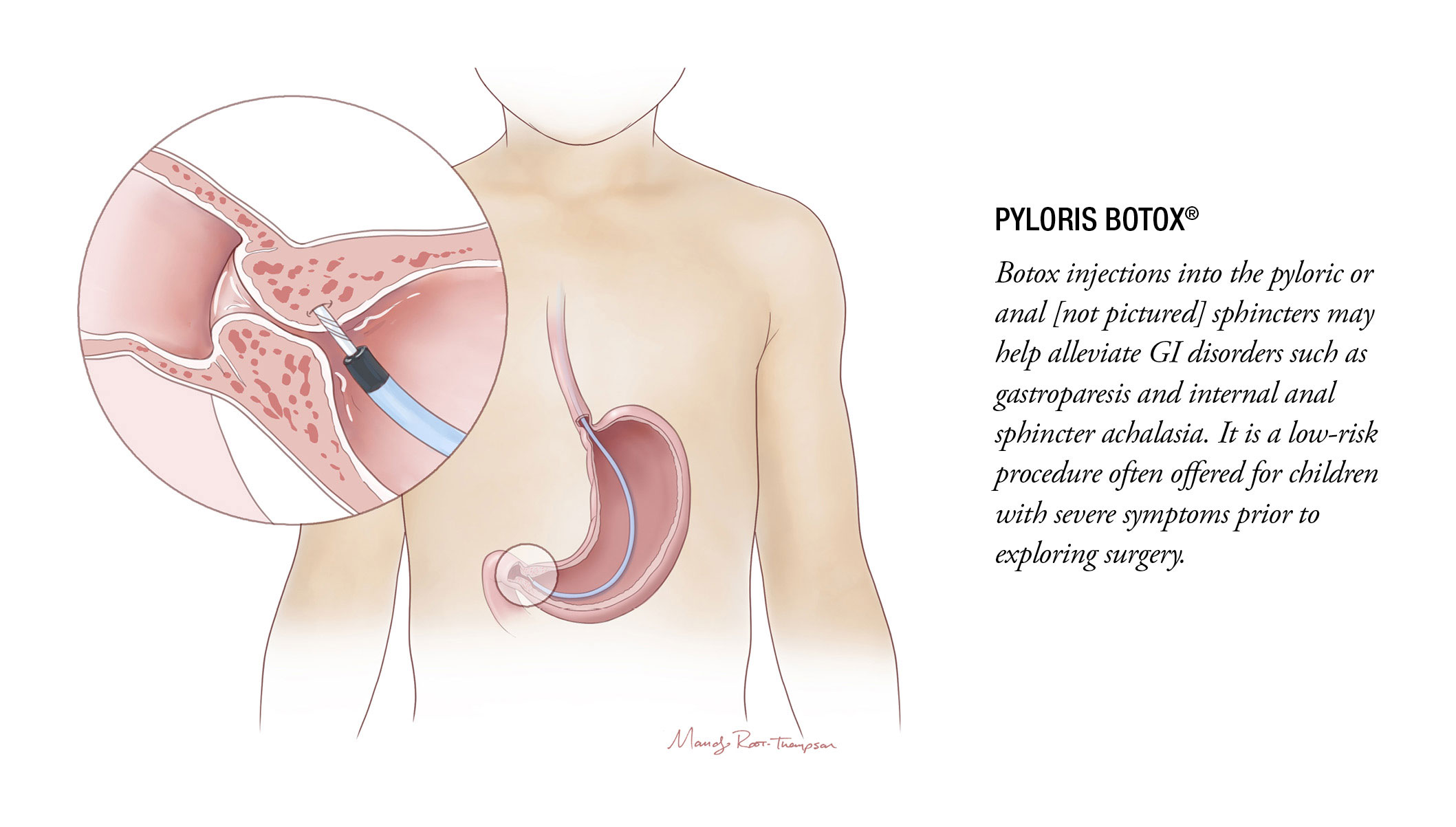
It’s true. Botox® has a place in modern GI motility therapy for children with certain motility issues, such as Hirschsprung’s disease and delayed gastric emptying. In these cases, a quick Botox injection directly into the anal or pyloric sphincter, respectively, may offer sufficient muscle relaxation to improve motility.
Long used in the treatment of Hirschsprung’s disease, anal Botox is also appropriate in children with severe functional constipation, according to a 2019 Journal of Pediatric Surgery study by Nationwide Children’s physician-scientists. And although pyloric Botox requires an endoscopy, it is less invasive and carries fewer risks than many surgical procedures.
Injections in either sphincter often produce lasting responses, sometimes relaxing the muscles long enough for GI concerns to resolve entirely.
DIET
Many GI care programs now include dietitians to help manage the unique nutritional needs of patients with functional and motility disorders. From managing feeding tubes to the low-FODMAP diet (a diet plan low in the fermentable carbohydrates that create irritating gas in the GI tract) for children with irritable bowel syndrome (IBS), these highly specialized GI dietitians significantly impact the care of patients seeking to manage or even resolve sensitivity-related GI symptoms through dietary management.
The Nationwide Children’s GI nutrition team is currently working to publish data they presented at Digestive Disease Week in 2019 on the efficacy, safety and feasibility of the low-FODMAP diet for children with IBS.
“Especially for functional disorders like IBS, medications aren’t the only way to go – behavioral therapy and diet can be just as effective, if not more so,” says Peter Lu, MD, MS, a pediatric gastroenterologist and physician-scientist in the Center for Neurogastroenterology and Motility Disorders at Nationwide Children’s.
BEHAVIORAL AND PSYCHOLOGICAL THERAPY
“GI psychology is increasingly being recognized as helpful in a lot of contexts as a non-medical option to treat many functional and motility conditions,” says Ashley Kroon Van Diest, PhD, a pediatric psychologist at Nationwide Children’s. “GI psychologists help fill a lot of needs in patient care.”
Some GI conditions frequently coincide with anxiety, depression and increased sensitivity to pain, and even children without these problems often have psychosocial challenges – embarrassment about their symptoms, judgment or accusations from friends and family – that make this additional care beneficial.
“We do evaluations and provide treatment recommendations for the family, and explain that it’s not all in their heads – the pain and symptoms are very real,” says Dr. Kroon Van Diest.
Together, she and the treating gastroenterologist see all patients coming to the hospital’s Functional Gastrointestinal Disorders Clinic to determine diagnoses and optimal treatment plans. She may also recommend follow up with additional therapy and program services such as massage therapy, therapeutic recreation, nutrition and more.
“To help many of these children, you have to approach the problem from a biopsychosocial model,” says Desalegn Yacob, MD, medical director of the Center for Neurogastroenterology and Motility Disorders. “Psychologists have a huge role in treating these patients, not because they have classic psychological conditions, but because they can see patients’ environmental and psychosocial influences on their physical health, and address them with gut-directed therapy.”
Rumination Therapy
One diagnosis that benefits substantially from the involvement of psychological care is rumination syndrome, a rare GI disorder that makes it hard for children to consume anything by mouth without vomiting almost immediately due to learned but involuntary muscle contractions. Fortunately, rumination experts can work with children – some of whom have not kept down a bite of solid food for years and are reliant on feeding tubes – to teach them how to eat normally again.
Over the course of about a week, Dr. Kroon Van Diest, who is the lead psychologist for the pediatric Rumination Syndrome Program at Nationwide Children’s (the only one of its kind in the country), works with patients to retrain their muscles by dry swallowing again as soon as they feel their stomach start to contract. Children are also taught to use diaphragmatic breathing when they eat to relax the abdominal muscles and prevent the contractions that cause food to come up. The majority of patients leave the program no longer requiring feeding tubes.
“It’s a relatively short-term, intensive treatment, but we send them back home to school and sports and things they haven’t been able to do in years,” says Dr. Kroon Van Diest, who also has a study underway to expand the center’s current treatment outcome data, published in the American Journal of Gastroenterology in 2018, to a longer follow-up. “It’s very impactful and very rewarding.”
Cognitive Behavioral Therapy
Patients with pain-related conditions, such as IBS, may be offered cognitive behavioral therapy (CBT) to learn how to cope with and relieve some of their abdominal pain. With this psychology-led approach, children are taught strategies to activate the parasympathetic nervous system. This slows the heart rate and breathing, counteracting the body’s typical response to pain. As a bonus, the practice may distract children from focusing on their pain.
“Research shows that over the course of 6-8 weeks, children who practice CBT most days a week – even for very short periods each time – experience changes in the pain processing centers of the brain on fMRIs,” says Dr. Kroon Van Diest, who has research pending publication demonstrating similar effects of CBT on fMRI pain center activity in children with migraines. “Reduced pain center activity correlates with better school performance, a lower perceived pain score, improved functioning and other positive changes.”
Biofeedback Therapy
For patients with constipation and fecal incontinence, biofeedback can be used to teach children “defecation dynamics” – how to have a bowel movement. In the Motility Center’s Pelvic Floor Rehabilitation/Biofeedback program, Kimberly Osborne, CPNP-PC, meets with children to provide this form of behavioral therapy.
In each session, small electrodes placed around the patient’s stomach and/or anus are connected to a computer with an instructional screen. The nurse practitioner walks through how to relax and how to contract the area using the images on the screen. Over time, patients learn how to control the pelvic floor muscles in order to control defecation and relieve symptoms.
Members of the biofeedback team are working with a patient. Over time, the practice will help the patient learn how to control the pelvic floor muscles.
NEUROMODULATION THERAPY FOR GI ILLNESSES
No other treatment has generated as much excitement in the field of neurogastroenterology as neuromodulation – electric stimulation of the nerves to reduce pain, ease constipation and relieve nausea or other symptoms. And the experts believe this is just the beginning.
Gastric Electrical Stimulation (GES)
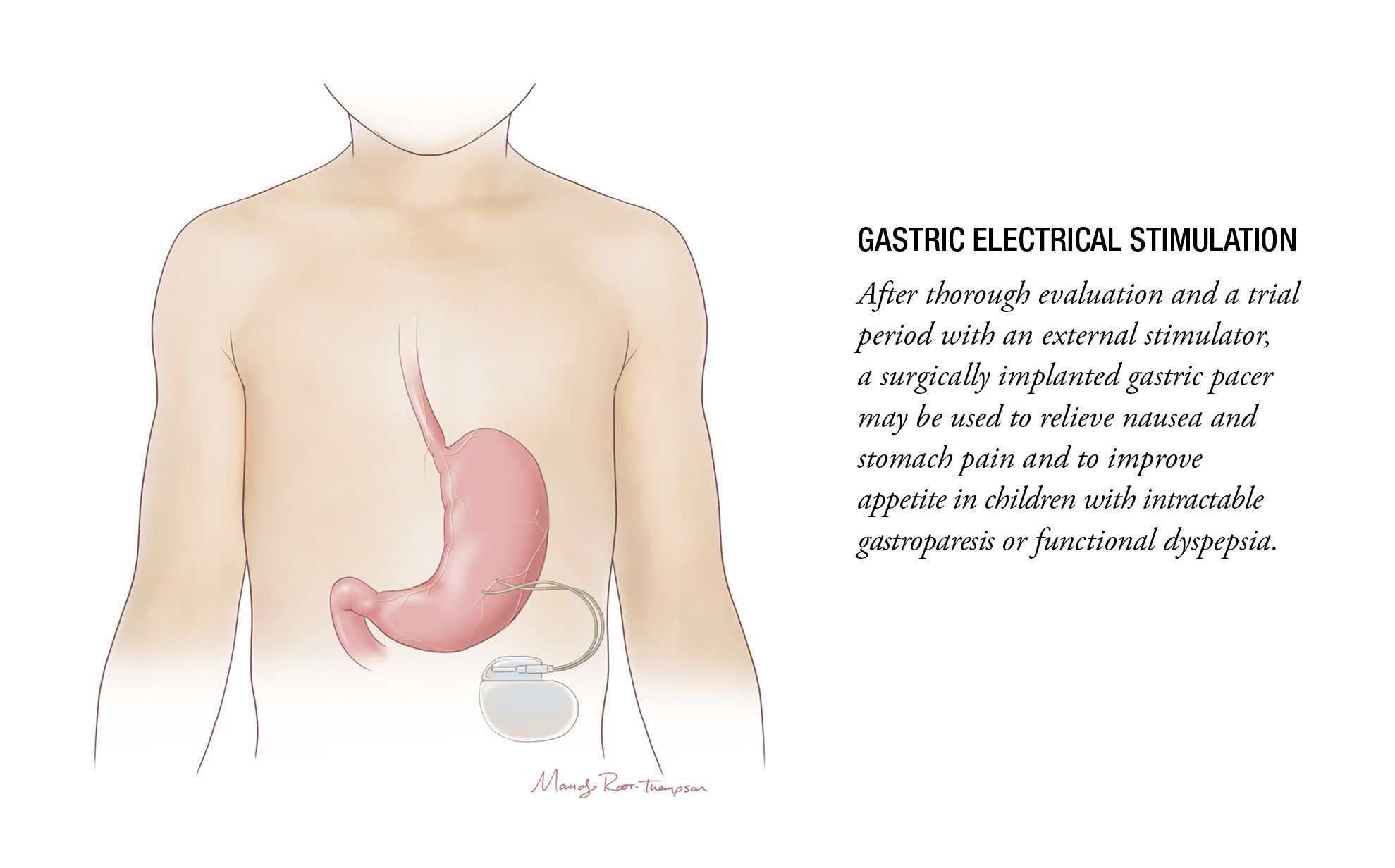
After other treatments fail, GES may be used in the care of severe nausea and abdominal pain caused by functional GI and motility disorders, such as gastroparesis and severe, intractable functional dyspepsia. Although its exact mechanism is not clearly understood, GES uses a device much like a pacemaker to provide gentle, frequent stimulation to the nerves of the stomach – not forcing the stomach muscle to contract or push food through, but perhaps numbing or calming the hypersensitive nerves.
Despite lacking a clear mechanism of action, GES often brings symptom relief, improving appetite regardless of any change in motility. Its external controls allow the device to be adjusted in strength and frequency of the stimuli, and many devices can stay in place 5-10 years prior to requiring reoperation to replace the battery.
“If children don’t respond to behavioral and lifestyle interventions or medication, often the only options left are surgical,” says Dr. Lu. “Neuromodulation has the advantages that – even though it can require surgery – it is usually adjustable and reversible, which is ideal for children.”
The Nationwide Children’s Motility Center is one of the country’s largest programs in terms of implant volume and neuromodulation research. The team is planning to publish 10 years of outcomes data (also presented at Digestive Disease Week this year) for the patients who have received one of the 85 gastric pacers placed by Nationwide Children’s GI motility experts and surgeons since 2009.
“We have had GES patients who could not tolerate anything – even a slow-drip feeding tube,” says Dr. Lu. “Literally a couple of months after the procedure, they could tolerate full feeds and wanted to eat.”
The motility team at Nationwide Children’s has begun using the procedure even in young children who qualify, and they have also developed an approach (called the CDiLo technique) to better secure the gastric pacer’s wire to the stomach during GES trials, allowing for a longer test period before permanent implantation.
“Seeing how patients respond to this intervention has been very rewarding, and it’s only a start,” says Dr. Yacob, who is optimistic that long-term outcomes data, expansion of eligible patient groups and advancement in understanding of the mechanisms of GES will further cement its use in pediatric therapy. “I think there are a lot of patients who could benefit from this approach.”
Sacral Nerve Stimulation
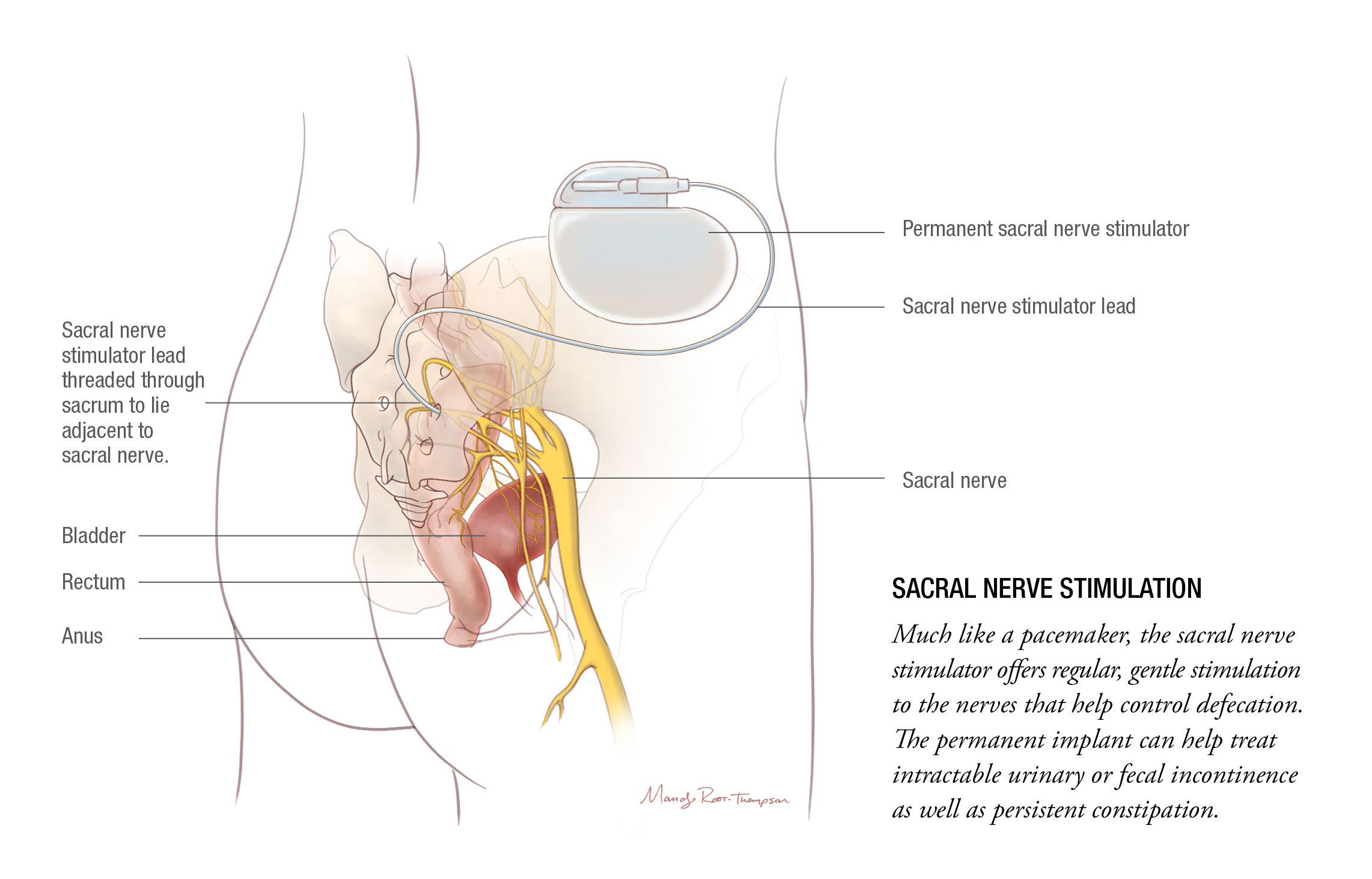
Although relatively new in the pediatric GI space, sacral nerve stimulation (SNS) has been offered for nearly a decade at Nationwide Children’s, starting in children with urinary incontinence and moving into cases of constipation and fecal incontinence.
Together, the urology and GI teams have implanted nearly 100 stimulators and have published regularly on their experiences with what is one of the largest SNS cohorts in the world. Recent work published in Neurogastroenterology and Motility has established its long-term efficacy in relieving constipation and fecal incontinence and has demonstrated that the procedure results in lasting parental satisfaction.
“I find the sacral nerve stimulation data published by the Nationwide Children’s motility group and the myriad of individual and collaborative clinical and research endeavors they have undertaken to be empowering,” says Lusine Ambartsumyan, MD, director of the Gastrointestinal Motility program at Seattle Children’s Hospital. “Their work paves the way for novel diagnostic and therapeutic innovations and allows other motility specialists to establish similar programs and protocols at their own institutions, to improve the care and the quality of life of our patients.”
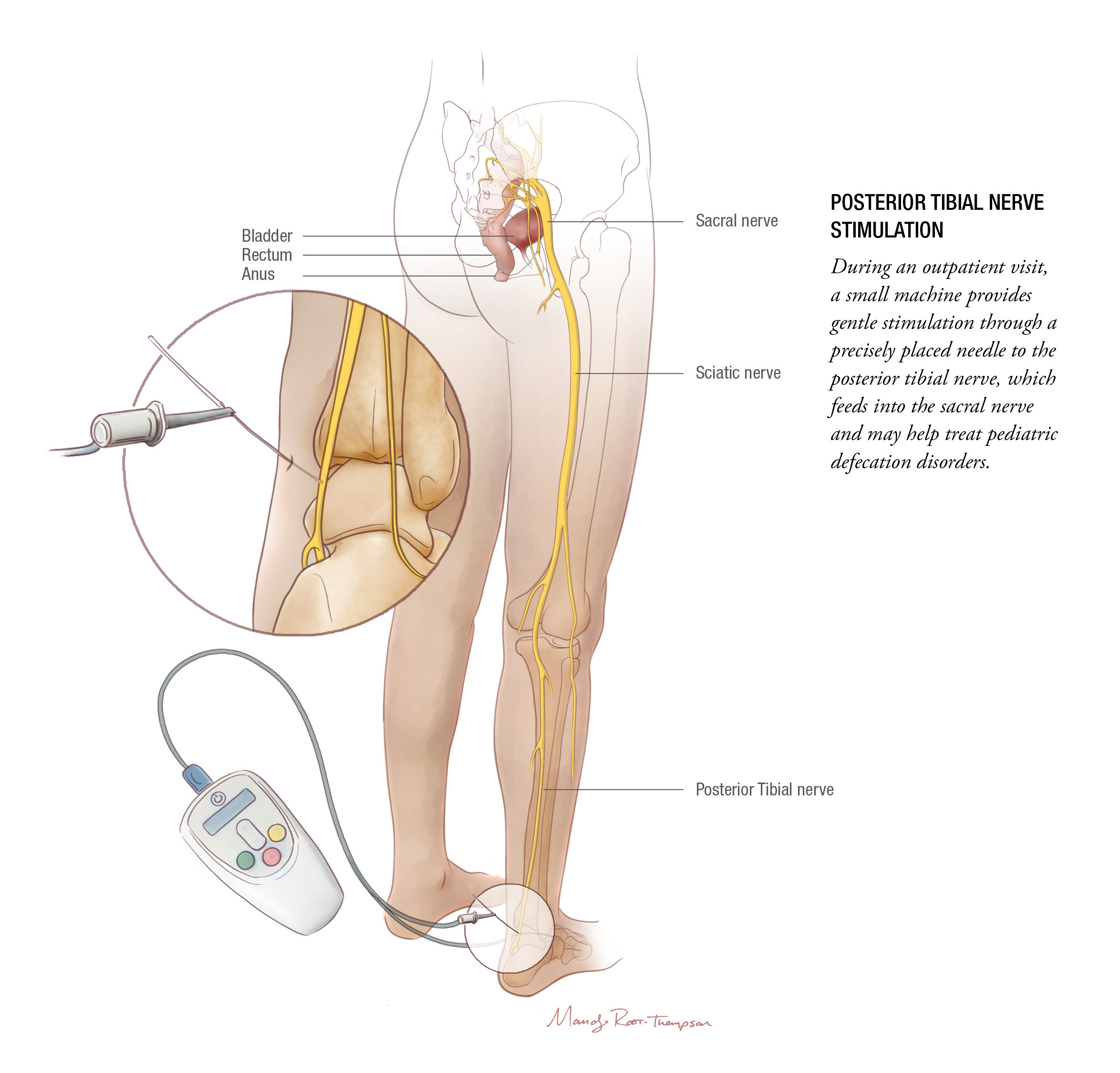
Posterior Tibial Nerve Stimulation
“We know from GES and SNS that electrostimulation of the GI tract can work,” says Dr. Lu. “But those approaches require implantation, so there is a lot of interest in how to do this without using a surgery.”
Like sacral nerve stimulation, posterior tibial nerve stimulation (PTNS) stimulates the nerve that feeds into the sacral nerve roots, which control bladder and bowel function. Although used for several years in the world of urology, PTNS for pediatric constipation and fecal incontinence is still under the umbrella of clinical research. Dr. Lu and his colleagues suspect it acts on the anorectal area rather than higher up in the colon, which would suggest that children with constipation due to anorectal or pelvic floor issues may respond the best.
“Even if sacral nerve stimulation is slightly more effective,” Dr. Lu says, “PTNS is noninvasive – a huge advantage.”
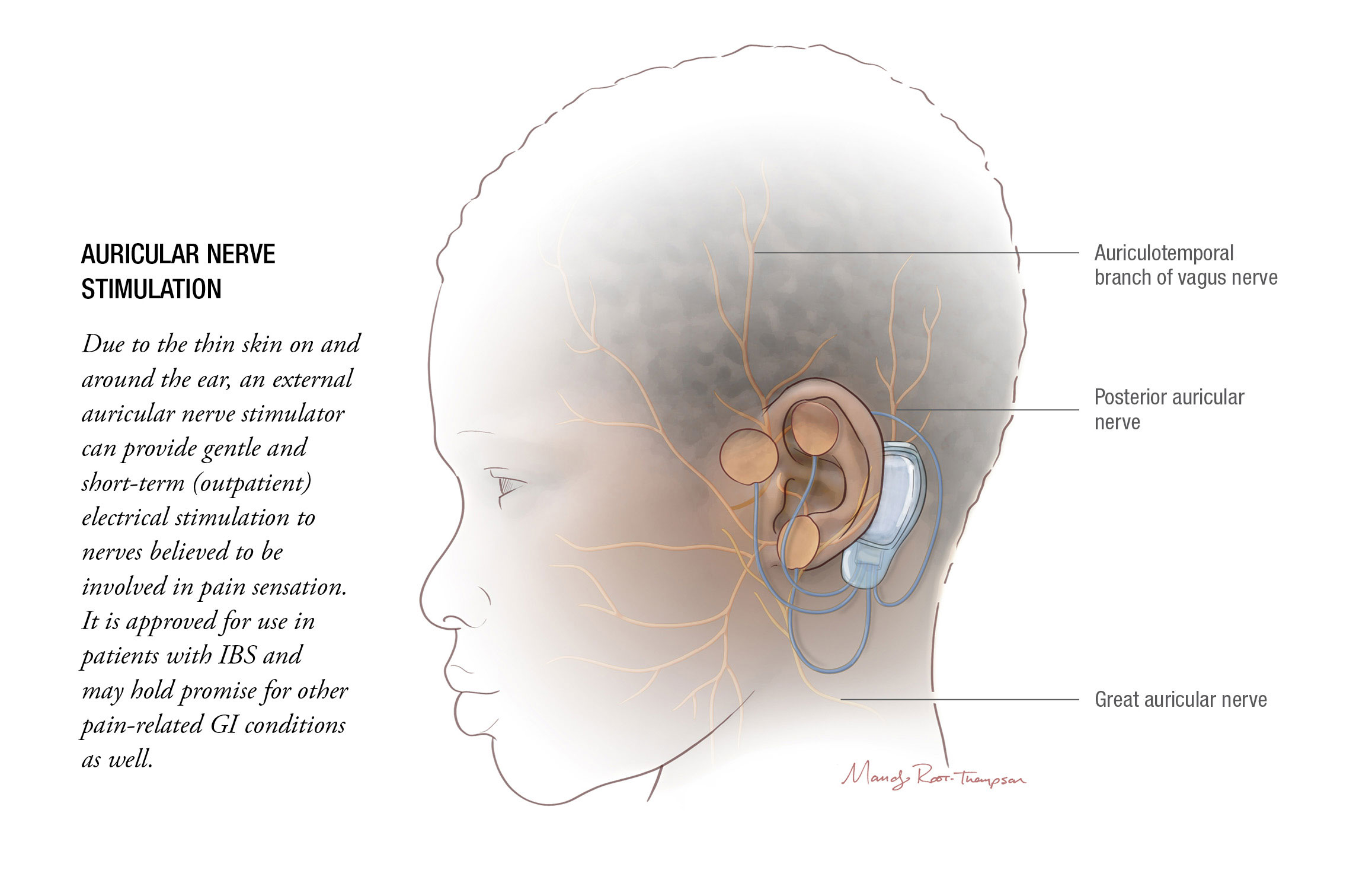
Auricular Nerve Stimulation
Recently approved by the FDA for the treatment of IBS, an electrical device called IB-Stim produces gentle stimulation of the auricular nerves, located just under the skin in the ear. While the exact mechanism is not fully understood, pain relief appears to result from the electrical impulses’ influence on the amygdala and spinal cord, and possibly other pain-control areas in the central nervous system.
The clinicians in the Motility Center are complimentary about the technology and believe it has a valuable place in the treatment paradigm for IBS.
“The idea of stimulating the ear or ankle and making your GI tract work better is very intriguing, and it helps a lot of people feel better with no side effects,” says Dr. Di Lorenzo. “These interventions differ from surgery and drugs in that, if they don’t work for you, you haven’t lost anything.”
COLLABORATING FOR THE FUTURE
Taken together, the growing range of treatment options for functional and motility disorders offers patients unprecedented opportunities for clinical improvement.
“When it comes to both research and care, we do it as a group,” says Dr. Yacob. He, Dr. Di Lorenzo, Dr. Lu and attending pediatric gastroenterologists Karla Vaz, MD, MEd, and Neetu Bali, MD, MPH, complete the team of five motility specialists, who also work with a Motility Center nurse practitioner, physician assistant, four dedicated nurses and two administrators. The team collaborates with pediatric surgeons, urologists, psychologists, dietitians, interventional radiologists and other experts to develop and discuss evaluation and treatment plans with each new patient. “We always try to focus on what is relevant and could help change how we treat these patients, then do our best to share our findings with colleagues around the country.”
Learning from other leading motility experts, such as Dr. Ambartsumyan, is crucial for continuing advancements, as well. Her use of 3-D high-definition anorectal manometry to better characterize the intra-anal pressure profiles of children with a normal anorectum and in those with anorectal malformations, published originally in the American Journal of Gastroenterology with another submission pending, should improve physiologic assessment of function in children with anorectal malformations who suffer from fecal incontinence. In time, she expects it will also help clinicians better tailor their treatment approaches for these patients.
Dr. Ambartsumyan is not alone in her potential to impact the future for children with functional and motility disorders. Other experts, as well as fellows trained through Nationwide Children’s functional and motility fellowship, are feverishly working to carry the knowledge currently concentrated in a handful of specialty centers to other burgeoning motility programs, increasing access to care for children at institutions closer to their homes.
“The field of functional and motility disorders is in a much better place than it was 20 years ago,” says Dr. Di Lorenzo. “There is still room for improvement, but by working together, we’re definitely getting better.”
References:
- Alioto A, Di Lorenzo C. Long-term follow-up of adolescents treated for rumination syndrome in an inpatient setting. Journal of Pediatric Gastroenterology and Nutrition. 2018 Jan;66(1):21-25.
- Ambartsumyan L, Rodriguez L, Morera C, Nurko S. Longitudinal and radial characteristics of intra-anal pressures in children using 3D high-definition anorectal manometry: New observations. American Journal of Gastroenterology. 2013:108:1918–1928.
- Halleran DR, Lu PL, Ahmad H, Paradiso MM, Lehmkuhl H, Akers A, Hallagan A, Bali N, Vaz K, Yacob D, Di Lorenzo C, Levitt MA, Wood RJ. Anal sphincter botulinum toxin injection in children with functional anorectal and colonic disorders: A large institutional study and review of the literature focusing on complications. Journal of Pediatric Surgery. 2019 Apr 23. [E-pub ahead of print.]
- Holzmacher M, Wall J, Jones K, Kuhn L, Maltz R, Bali N, Baz K, Yacob D, Di Lorenzo C, Lu PL. [Mo1548] Efficacy, feasibility, and safety of the low FODMAP diet for children with irritable bowel syndrome: A prospective cohort study and phone survey. Gastroenterology. May 2019;156(6):S-776.
- Lu PL, Koppen IJN, Orsagh-Yentis DK, Leonhart K, Ambeba EJ, Deans KJ, Minneci PC, Teich S, Diefenbach KA, Alpert SA, Benninga MA, Yacob D, Di Lorenzo C. Sacral nerve stimulation for constipation and fecal incontinence in children: Long-term outcomes, patient benefit, and parent satisfaction. Neurogastroenterology and Motility. 2018 Feb;30(2).
- Lu PL, Mousa HM. Constipation: Beyond the old paradigms. Gastroenterology Clinics of North America. 2018 Dec;47(4):845-862.
- Lu PL, Teich S, Di Lorenzo C, Skaggs B, Alhajj M, Mousa HM. Improvement of quality of life and symptoms after gastric electrical stimulation in children with functional dyspepsia. Neurogastroenterology and Motility. 2013 Jul;25(7):567-e456.
- Ryan K, Orsagh-Yentis D, Diefenbach KA, Teich S, Mousa H, Bali N, Vaz K, Yacob D, Di Lorenzo C, Lu PLL. [758] Long-term outcomes of gastric electrical stimulation for children with severe nausea and vomiting: A ten-year experience. Gastroenterology. May 2019;156(6):S-157.
Image credits: Mandy Root-Thompson for Nationwide Children’s
About the author

Katherine (Katie) Brind’Amour is a freelance medical and health science writer based in Pennsylvania. She has written about nearly every therapeutic area for patients, doctors and the general public. Dr. Brind’Amour specializes in health literacy and patient education. She completed her BS and MS degrees in Biology at Arizona State University and her PhD in Health Services Management and Policy at The Ohio State University. She is a Certified Health Education Specialist and is interested in health promotion via health programs and the communication of medical information.
- Katie Brind'Amour, PhD, MS, CHEShttps://pediatricsnationwide.org/author/katie-brindamour-phd-ms-ches/

- Katie Brind'Amour, PhD, MS, CHEShttps://pediatricsnationwide.org/author/katie-brindamour-phd-ms-ches/
- Katie Brind'Amour, PhD, MS, CHEShttps://pediatricsnationwide.org/author/katie-brindamour-phd-ms-ches/
- Katie Brind'Amour, PhD, MS, CHEShttps://pediatricsnationwide.org/author/katie-brindamour-phd-ms-ches/


