
Better Asthma Outcomes: A Systems-Level Approach
Better Asthma Outcomes: A Systems-Level Approach https://pediatricsnationwide.org/wp-content/uploads/2025/09/101824BT0901-header-for-web-1024x422.jpg 1024 422 Katie Brind'Amour, PhD, MS, CHES https://pediatricsnationwide.org/wp-content/uploads/2021/03/Katie-B-portrait.gif
A dedicated team of experts embraced sweeping tactics to reduce asthma-related emergency department visits by 33% and inpatient length of stay by 0.9 days. This is how they did it.
It started with a conversation about the data: Why are kids with asthma the hospital’s most frequent fliers? After all, excellent preventive and acute treatments exist for asthma. Properly managed asthma should have minimal impact on a child’s well-being.
And there’s the rub.
Asthma requires consistent attention. Families must understand how to avoid asthma triggers, how to recognize symptoms, what medications to use and when, how to administer the correct dose, when to refill prescriptions and how to manage and avoid asthma flares.
A short visit to the hospital often involves different medications and management strategies than families use at home, which can leave families unprepared to effectively transition back to self-care. To complicate matters, primary care physicians may not be familiar enough with the reasoning behind prescription changes to effectively guide maintenance regimens moving forward.
Together, these challenges make an otherwise straightforward medical condition a monumental hurdle from a population health standpoint, especially because asthma affects as many as 6-10% of all children. Not surprisingly, perhaps, asthma has historically been the most common diagnosis for inpatient hospitalizations at Nationwide Children’s Hospital.
The idea of a systems-level, multilayered approach to the management of a common pediatric health condition sounds ideal, but in practice, there are often too many moving parts — and competing priorities — to make headway.
But that’s exactly what a dedicated team at Nationwide Children’s has done over the past 15 years, resulting in dramatic transformations in pediatric asthma outcomes in central Ohio.
In the process, asthma fell from being the No. 1 most common diagnosis for hospital admissions to No. 3.
Building the Asthma Core Team
In 2010, asthma’s place at the top of the chart for inpatient admissions at Nationwide Children’s — coupled with its inclusion in the hospital’s strategic plan to improve community health — prompted hospital administrators and their pediatric accountable care organization, Partners For Kids® (PFK), to ask pulmonologist Beth Allen, MD, now retired, to initiate a quality improvement (QI) plan to improve asthma outcomes. PFK manages care for more than 446,000 Ohio children on Medicaid and promotes chronic disease management.
Dr. Allen worked with the PFK team and consulted other pulmonologists, emergency medicine physicians, hospitalists, respiratory therapists and primary care specialists. As stakeholders across the care continuum agreed to join forces, the Asthma Collaborative was born. Over time, they assembled a Core Team composed of 33 members devoted to the team’s vision: helping children live a life not limited by asthma.
Together they would work toward the overarching mission of the Collaborative — with a reduction in emergency and inpatient visits related to asthma as the first common goal — sharing their plans and results in monthly meetings. Independently, they would set discipline-specific QI projects and implement changes in their own departments.
This cross-disciplinary, multi-tiered approach was essential.

Lisa Ulrich, MD
“Seeing patients as a pulmonologist, we have one small point of view — we don’t get to see what happens everywhere else,” says Lisa Ulrich, MD, pediatric pulmonologist and medical leader of the Asthma Core team at Nationwide Children’s since 2021. “We are fortunate we have experts from each area who take part. The Core Team members help figure out the best ways to adapt interventions and get buy-in from their own departments. There isn’t one person forcing something to fit into a box when their department is really a circle.”
Primary Care as the Primary Focus
Primary care physicians perform the vast majority of asthma diagnosis and management.
“We pride ourselves on having a discussion about asthma often with our patients,” says Stephen Hersey, MD, primary care pediatrician and co-lead of the Primary Care Network asthma QI team. Prior to the launch of the Asthma Collaborative, he worked to roll out asthma guidelines in clinical practice for primary care centers in Ohio as part of his QI work for the Ohio Chapter of the American Academy of Pediatrics.
As Dr. Hersey’s QI efforts merged with the hospital’s initiatives through the Collaborative, the primary care network — consisting of 14 clinics and about 100 physicians — adopted a plan with five key goals:
- Incorporate customizable asthma action plans into the electronic medical record (EMR) and achieve 80% completion rates.
- Launch asthma specialty clinics staffed by primary care pediatricians with extended length visits for patients requiring more complex asthma care or intervention, and average 250 visits per month.
- Increase completion of asthma notes (standardized EMR-based forms designed to promote guideline-based care and discussion of asthma status) from 20% to 65% of all encounters with asthma patients, regardless of the reason for the visit.
- Increase documentation of an asthma control test (ACT) from 40% to 70% of all encounters with asthma patients, regardless of the reason for the visit.
- Standardize approaches to step-up therapy and increase referrals to support resources for children with poorly controlled asthma from 35% to 50%.
The five initiatives rolled out gradually from 2011 to 2015, and their results were remarkable.
In a population of 86,356 patients, of whom 10% had asthma, asthma-related ED visits fell from 21.7 per 1,000 patients per year in 2010 to 14.5 per 1000 patients per year in 2019 — a 33% reduction. Asthma action plan documentation went from 0% to their goal of 80%, and asthma control test records nearly doubled, achieving the 70% target. They published their results in Pediatrics.
The team has also maintained at least a 50% rate of appropriate medication escalation and guideline-based step-up strategies for patients with poorly controlled asthma. Visits to the specialty clinic hit the target but subsequently reduced to an average of about 176 per month.
To make these changes possible, Dr. Hersey and co-leader of the asthma QI team Jessica Retzke, MD, visited each primary care clinic for initial training and continue to onboard new residents and physicians. They both have one day a week dedicated to their QI work, and receive extensive data analysis support from the hospital’s Asthma Core Team QI guru, Charles Hardy, MHA, CPHQ, lead quality strategist at Nationwide Children’s, who supplies them and the rest of the Collaborative with overarching data. Care providers get regular individual and clinic-specific reports to indicate performance on key asthma metrics.

Stephen Hersey, MD
“When I joined Nationwide Children’s in 2007, if I had to step a kid up off of Flovent [an inhaled corticosteroid] because their asthma was not controlled, I would refer to pulmonology,” Dr. Hersey says. “After working on these projects, I can see my evolution as a practitioner. Now our network providers, including younger faculty and nurse practitioners, have an increased level of confidence from using our embedded processes, and quickly become comfortable stepping up therapy.”
EMR best practice alerts categorize children into low-, medium- and high-risk groups with relevant program referrals suggested according to identified risk factors. At least half a dozen other asthma-related alerts prompt other actions to improve asthma outcomes.
But even with better action plans and optimized prescriptions, some families need more support.
Bringing Asthma Care Straight to Patients

Loan (Kathy) Nguyen, PCPNP
“I used to work in primary care and had the mentality that we’d meet with the family, give them the action plan, send in the prescription and send them on their way thinking that’s what they’d do,” says Loan (Kathy) Nguyen, PCPNP, program coordinator of School-Based Asthma Therapy (SBAT), which serves about 1,000 children at more than 300 schools in the greater Columbus area. “Working for SBAT has changed my mindset about asthma, health barriers and health equity. There are so many things families face that can make it hard to give a controller medication every day.”
Some families have no car to get to the pharmacy or don’t know how to refill a prescription. Insurance coverage changes and prices go up, making things too expensive. They mix up controller and rescue inhaler instructions. Kids split their time between two households. Or parents work in the morning, leaving children responsible for taking their own daily maintenance medication before school.
Schools and clinicians refer kids with absences and illness due to asthma to SBAT, and SBAT nurses collaborate with school nurses or office staff to administer daily preventive medications at school. SBAT nurses coordinate delivery of prescriptions straight to the school. They also work to increase communication between the family, school and asthma provider about asthma concerns — such as increased symptoms, hospital utilization and suggestions on possible medication changes — in order to come up with a plan that optimizes asthma control.
Within a year of SBAT enrollment, 37% of children newly achieved well-controlled asthma according to the Asthma Control Test and 56% according to health care provider ratings, as published in the Journal of Allergy and Clinical Immunology: Global. Asthma-related ED visits and inpatient admissions each dropped by 50% among participants, intensive care unit (ICU) admissions fell by 71%, and acute and urgent visits fell by 38% and 41%, respectively. Improvements were even greater for certain indicators among Black and Latino children and have obvious implications for children’s ability to attend school.
“SBAT is really helping kids who otherwise would fall through the cracks and probably be very ill if they weren’t getting that oversight and assistance with adherence to their medications at school,” says Nguyen. “It has been a very beneficial program for our families.”
Impressed by the impact on utilization, PFK sought out additional funding to expand the SBAT program. A new grant will grow the SBAT provider team from nine staff members (primarily nurses) to 11 and increase patient capacity by 50% to serve more than 1,500 children.

Rajitha Venkatesh, MD
“Supporting our patients means truly understanding their lives and providing the specific resources they need to thrive,” says Rajitha D. Venkatesh, MD, MPH, FAAP, medical director for the Chronic Conditions service line at PFK. “The journey to staying out of the hospital is complex, and we’re here to help navigate every layer — from securing transportation and facilitating medication delivery to offering vital asthma education.”
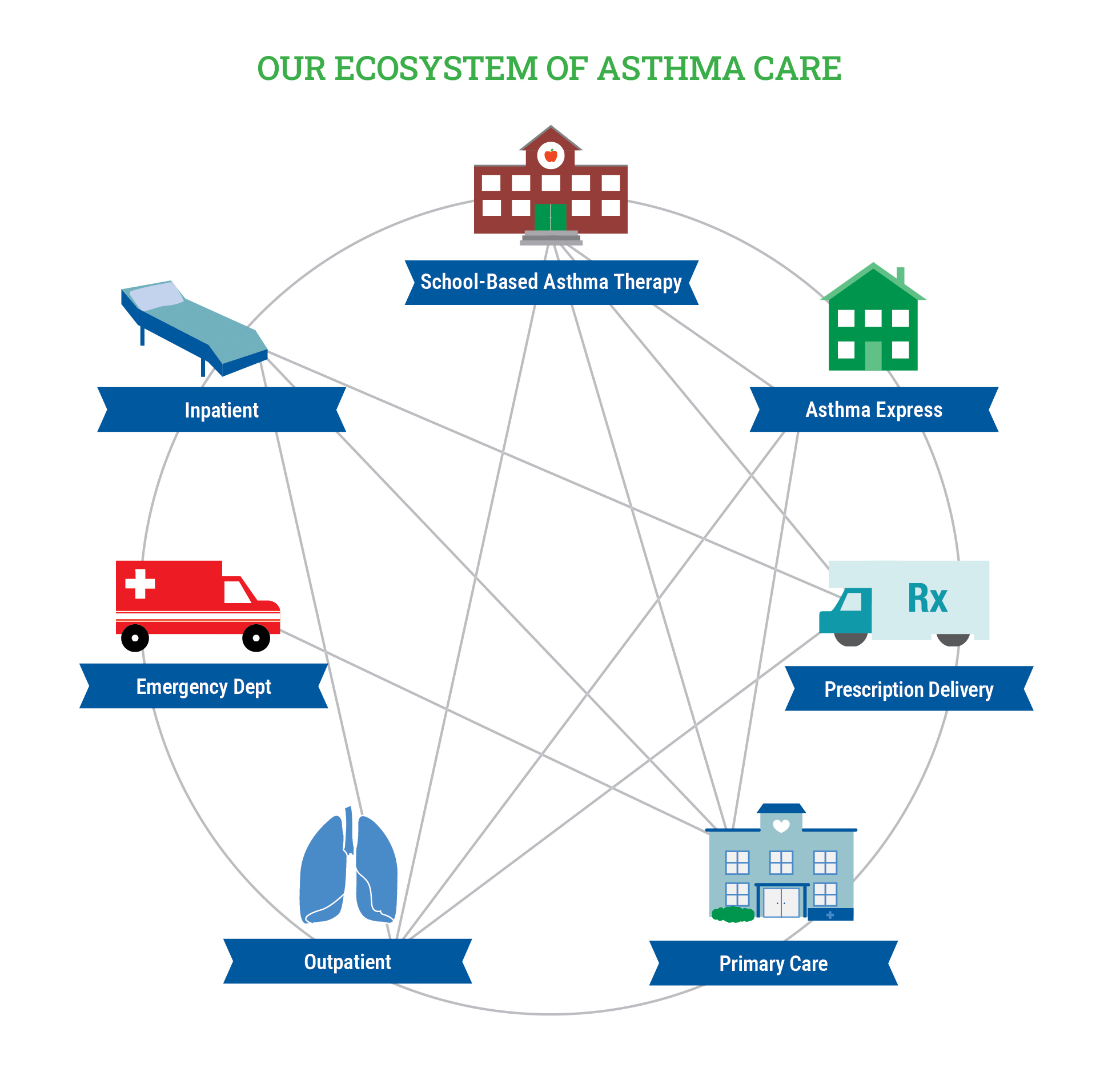
Families requiring further help at home can benefit from Asthma Express, a program that sends nurses to patient homes to evaluate and educate about medication, symptoms and asthma triggers. Prescription delivery services now also address barriers in access to pharmacies by bringing medications straight to patients’ homes when needed.
Together with enhancements in primary care, these efforts have collectively made major contributions to reductions in asthma-related ED and inpatient admissions at Nationwide Children’s.
In Case of Emergency
While patient care prior to an exacerbation is outside the control of the ED itself, several QI plans aimed to reduce utilization and the cost of care within the walls of the hospital dovetail with efforts to standardize and streamline care across the continuum of providers.

Adjoa Andoh, MD
“A lot of our work in the ED is focused on better care for exacerbations, but we still ask for collaboration and ideas from the wider Core Team because what we do in the ED can impact what happens when patients go home or get admitted,” says Adjoa Andoh, MD, emergency medicine physician and leader of the ED asthma QI team at Nationwide Children’s.
The first plan the ED asthma QI team rolled out was steroid administration within 60 minutes of arrival at the ED for all asthma exacerbations. The metric aligns with national guidelines and results in shorter stays and fewer inpatient admissions — outcomes the team has ameliorated despite facing barriers to rapid steroid administration.
The ED asthma QI team has since implemented multiple complementary QI projects, two of which aim to increase their chances of achieving the overarching 60-minute steroids goal:
- The licensed practitioner initiation project, to increase the rate of steroids ordered by nurses during triage
- A paramedic steroid administration project, to increase steroid use en route to the hospital
- A nebulizer reduction project, now in sustain mode after effective replacement of high-albuterol nebulizers with more efficient equipment (described in a Pediatric Quality & Safety publication)
The ED receives about 2,000 asthma-related visits per year. As in other departments, changes to practice involve hundreds of people who all have other patients and diagnoses to manage as well, making stakeholder buy-in essential.
“Having that collaboration and getting the ideas and feedback from everyone that this touches is the only way to make any of these changes successful,” says Dr. Andoh.
Dr. Andoh has also looked beyond ED-specific metrics to improve asthma care. For one initiative, published in The Journal of Asthma, she examined national data to demonstrate the ability to cost-effectively and safely care for patients needing continuous nebulized albuterol on the regular inpatient floor after admission, rather than sending patients to the ICU. Because of her involvement in the Asthma Collaborative, her hospitalist colleagues were ready and willing to explore that practice change.
Inpatient and Outpatient Expertise
“Historically, continuous albuterol aerosols have been an ICU-level intervention, but our goal is to offer it for certain inpatients to prevent their transfer to the ICU for that intervention alone,” says Shauna Schord, MD, pediatric hospitalist at Nationwide Children’s and co-lead of the inpatient asthma QI team.
The inpatient team has already completed stepwise implementation of the measure with more than 40 patients and have a manuscript submitted for publication detailing their efforts.
Most measures they implement, however, focus on getting patients back to baseline respiratory status (or better) as fast as possible, and keeping them out of the hospital long-term. During admission, hospitalists and pulmonologists evaluate and adjust the patients’ asthma care plans as needed to maintain better health moving forward. They discuss adherence and any changes in preventive treatment, and hand off to pharmacists and respiratory therapists to enhance the education families receive before heading home.
“Our team has had longstanding goals that primarily surround our safety and efficiency in discharging patients home,” says Dr. Schord.
These include reducing length of stay and 30-day readmission rates to meet or beat national averages. Their efforts have dropped average length of stay from 2.4 to 1.5 days, and the team typically outperforms national averages for readmissions.
“Prior to being part of the Collaborative, I was more focused on acute management and the parts of care that I have direct control over,” says Karen Allen Glenn, MD, pediatric hospitalist at Nationwide Children’s and co-lead of the inpatient asthma QI team. “Now I think of asthma as a more chronic life problem that families need education to manage long term; my approach is more family-centered.”
Drs. Schord and Allen Glenn have attempted to promote this shift in mindset among the other 60 hospitalists as well as the residents, nurses, respiratory therapists and pharmacists taking care of inpatients. They meet regularly to discuss failures and successes and to identify any aspects of care that prevent rapid improvement or prompt discharge.
They recently identified completion of the updated asthma action plan and physician decisions about discharge maintenance medications as bottlenecks in the discharge process; education and referrals to community resources cannot be completed until these changes happen, making their next QI target clearer.
Big Goals, Big Actions, Big Impact
Beyond the efforts directed at patient education and experience, PFK operates behind the scenes to produce policy and payer-level changes to further impact families coping with asthma.
Pharmacy leaders in the program advocated for continued coverage of key asthma drugs at a time when they were scheduled to be dropped from the Medicaid formulary, for example, resulting in continued access to critical controller medications for thousands of patients. The team also successfully lobbied to get coverage for two inhaler spacers per year per patient — an essential aid in proper drug delivery.
“We have a wide range of QI initiatives, including provider education, patient tools and resources, a PFK newsletter and Asthma Toolkit for providers, webinars and even an ECHO series to improve primary care provider knowledge and capabilities state-wide,” says Melanie Pinnow, MSN, RN, CCM, clinical director of the Chronic Conditions service line for PFK. “We provide care coordination and disease management services at the highest level.”
Despite having achieved the vast majority of their goals, members of the Asthma Collaborative see no end to their mission.
“Everybody is focusing on the next goals, working to create and streamline telehealth services to improve access to care and increase our focus on health literacy, education and teach-back methods,” says Amanda Truex, MS, RRT, AE-C, respiratory therapist and the asthma program coordinator at Nationwide Children’s. Teach-back implementation, which has been shown to improve patient adherence and confidence in disease management, has already increased by 20%.
In primary care, Dr. Hersey envisions a future where primary care providers conduct more advanced asthma care with the input of the Nationwide Children’s pulmonology team.
“Looking ahead, we aim to partner with specialists to ensure routine co-management of our patients, recognizing that their limited availability makes it challenging for them to see every child on a quarterly basis,” says Dr. Hersey.
In the ED, Dr. Andoh has research underway to support a change in the type of steroid used for exacerbations to try to reduce side effects and the number of doses required. Inpatient hospitalists aims to roll out non-ICU continuous nebulizer therapy to all eligible patients.
As family services grow across Ohio and early administration of steroids for exacerbations increases, inpatient admissions may drop even further.
“I have asthma, and my life mission when I chose to become a pulmonologist was to try to improve outcomes for kids with asthma,” says Dr. Ulrich. “I know what it feels like to not be able to breathe due to your asthma and want to prevent as many kids as I can from having to experience that themselves.”
With the Asthma Core Team hard at work, she may just see her dream come true.
This article appeared in the 2025 Fall/Winter print issue. Download the issue here.
References:
- Andoh AA, Hardy C, Evans L, Milem A, Whitacre C, Rust L, Masa A, Stewart G. Decreasing the use of albuterol nebulizer solution in the management of asthma exacerbations in the emergency department. Pediatric Quality & Safety. 2025 May 22;10(3):e814.
- Arcoleo K, McGovern C, Allen E, Irwin MK, Musmulyono M, Dela Cruz I, Walsh A, Noyes K, Veazie P, McGregor H, Harden SM, Halterman JS. School-based asthma therapy: Improving medication adherence, asthma control, and health care utilization. Journal of Allergy and Clinical Immunology: Global. 2025 Jan 31;4(2):100428.
- Hersey SJ, Retzke J, Allen ED, Snyder D, Hardy C, Groner J. A primary care-based quality improvement project to reduce asthma emergency department visits. Pediatrics. 2023 Dec 1;152(6):e2023061355.
Image credits: Nationwide Children’s
About the author

Katherine (Katie) Brind’Amour is a freelance medical and health science writer based in Pennsylvania. She has written about nearly every therapeutic area for patients, doctors and the general public. Dr. Brind’Amour specializes in health literacy and patient education. She completed her BS and MS degrees in Biology at Arizona State University and her PhD in Health Services Management and Policy at The Ohio State University. She is a Certified Health Education Specialist and is interested in health promotion via health programs and the communication of medical information.
- Katie Brind'Amour, PhD, MS, CHEShttps://pediatricsnationwide.org/author/katie-brindamour-phd-ms-ches/

- Katie Brind'Amour, PhD, MS, CHEShttps://pediatricsnationwide.org/author/katie-brindamour-phd-ms-ches/
- Katie Brind'Amour, PhD, MS, CHEShttps://pediatricsnationwide.org/author/katie-brindamour-phd-ms-ches/
- Katie Brind'Amour, PhD, MS, CHEShttps://pediatricsnationwide.org/author/katie-brindamour-phd-ms-ches/


