
Beyond the Wow Factor: Artificial Intelligence in Pediatrics
Beyond the Wow Factor: Artificial Intelligence in Pediatrics https://pediatricsnationwide.org/wp-content/uploads/2023/04/AdobeStock_552748421-1024x576.jpeg 1024 576 Katie Brind'Amour, PhD, MS, CHES https://pediatricsnationwide.org/wp-content/uploads/2021/03/Katie-B-portrait.gif
What promise do AI and machine learning hold for pediatrics, and how can their potential flourish while still safeguarding children’s health and privacy?
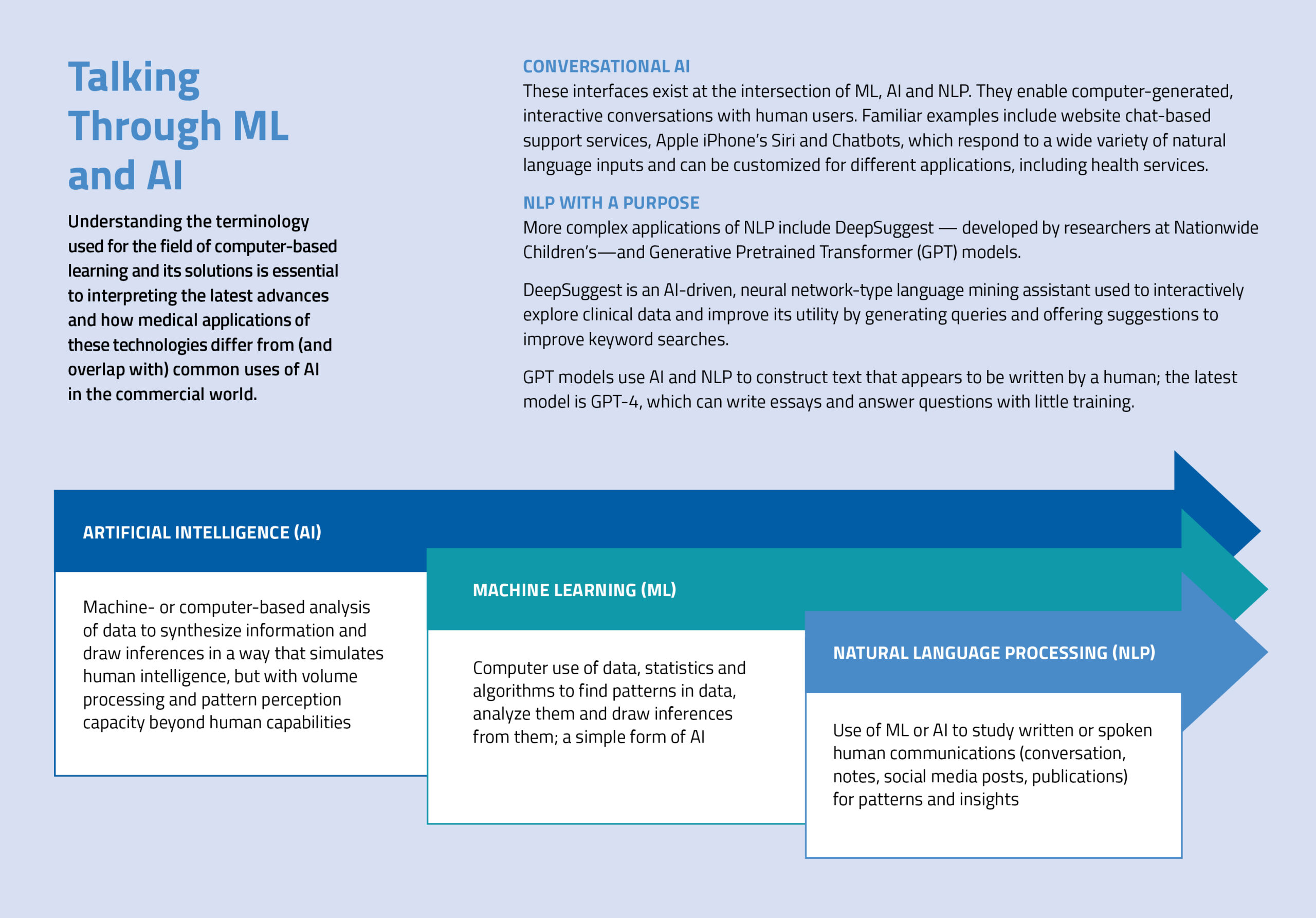
Machine learning (ML) and artificial intelligence (AI) have exploded across the worlds of marketing and commerce in recent years. Streaming services track what you watch and suggest other content you may enjoy. Sales algorithms identify your shopping patterns and make age-appropriate toy recommendations for your kids over time. There’s also a good chance you’ve read a sales letter or blog post and never suspected its author was a computer.
As ML and AI enter the world of health care and biomedical research, what are the most promising applications of computer-assisted decision-making, and how far are we from bringing these tools to daily clinical care? Where does the utility of AI end and the threat to human privacy or wellbeing begin? And what issues arise specific to pediatric applications of this technology?
A Brave New World For Medicine
Proponents of AI in medicine often refer to the world of computer-based insights as “augmented” intelligence — something supplemental and human-managed that can help improve decision-making, not an entity that operates independently or overrules a physician’s decision for patient care. In short, they view it as just another tool in the clinician’s tool belt.
This concept of AI is both reassuring and cautionary. It asserts that computer programs are not meant to replace physician judgment in clinical care, while requiring that its users understand AI’s findings, their reliability and the best way to utilize them.
When we implement AI in health care settings, we have to be extremely diligent. We need to know the weaknesses up front, watch it at every step, and build in complete transparency. Even after we have a model that we think is good enough, we implement it in the background and monitor it another 6 months to make sure it does what we want it to do.”
– Christopher Bartlett, PhD, principal investigator in the Steve and Cindy Rasmussen Institute for Genomic Medicine at Nationwide Children’s Hospital
At its present best, AI can accurately review a database of histology images and linked clinical data to formulate new prognostic criteria or stratify cancer by subtypes, all by detecting subtle details or drawing big data-based connections not feasible for humans to do manually.
In many other settings, application of this technology is in its nascent stages. At Nationwide Children’s Hospital, for example, clinicians and researchers are using ML to figure out how early, subtle changes in coronary blood flow patterns can predict the eventual development of coronary microvascular disease. The idea is that potentially valuable information may be present outside of what physicians can observe in echocardiograms and clinical data to indicate early, potentially modifiable physiological risk factors for future disease.
To this end, Aaron Trask, PhD, FAHA, FCVS, principal investigator in the Center for Cardiovascular Research at Nationwide Children’s, and experts including Christopher Bartlett, PhD, principal investigator in the Steve and Cindy Rasmussen Institute for Genomic Medicine at Nationwide Children’s collaborate to “train” their imaging-based ML model. This involves adjustments to the model so that it doesn’t rely purely on known risk factors for microvascular disease (such as diagnosed diabetes in the clinical file) but goes beyond, to data that humans may not be able to identify. It requires a large data set — gathered meticulously over several years and hundreds of imaging studies — and a lot of patience as the model learns to ignore things, such as the black space in the background of an echocardiogram image.
“Everything had to be analyzed in the traditional way and then fed into the data system, and then there has been a lot of back and forth to make sure the model has what it needs to learn something useful,” says Dr. Trask, who has been working with Dr. Bartlett and William Ray, PhD, an expert in data visualization at Nationwide Children’s, for several years to optimize the model. The latest improvements are described in Scientific Reports.
“At the end of the day, clinicians need to understand what factors the model is using to make its predictions,” says Dr. Trask. “It can’t be a black box to them, or physicians won’t be able to rely on it for their own decision-making.”
Beyond the contribution to accurate, informed decisions via better image processing and predictive profiling, ML and AI offer the opportunity to reduce clinician workloads and even enhance the care experience for patients.
Through a technique called natural language processing (NLP), advanced ML and AI applications are being trained to identify key details from in-office conversations for consolidated inclusion in medical records. According to Emre Sezgin, PhD, principal investigator in the Center for Biobehavioral Health at Nationwide Children’s, NLP techniques could not only save physicians and medical assistants hours each day in note-taking, they may also be used to identify and call to attention historical notes that could be relevant to an in-progress or upcoming consultation.
NLP exploration of notes in medical records can also reveal valuable community- or population-level insights: patterns in pre-diagnostic symptoms for a particular disease, implicit bias on behalf of providers and even age-, gender- or ethnicity-based trends in describing certain symptoms that can be used to help physicians identify problems earlier in the disease course.
Beyond these applications, ML and AI are exploding in niche areas of medical science, from genomic analysis to truly personalized oncology therapy. What remains to be seen is which of the many forms of these technologies will end up in the clinic once factors of infrastructure, cost, patient acceptability, regulatory approval and clinical utility are defined.
Practical Adoption Of AI In Pediatrics
As with most technologies, AI and ML have pros and cons. For example, ML requires many more data points than might be expected in order to come up with valid insights.
“I could train a 7-year-old to identify new things with three or four images,” says Dr. Bartlett. “But it can take tens of thousands of images or data points to train a machine learning model to reach the same conclusion, because it looks at absolutely everything and has to learn the hard way what is important and what isn’t.”
For adult cancers with common mutations, large data sets are relatively easy to obtain. But for children, who rarely get cancer and who tend to have unusual mutations, there may be very few samples or data points with which to train a model. This necessitates collaboration, and collaboration necessitates a common framework for structuring the data.
Enter the Bridge2AI Program, an initiative funded by the National Institutes of Health Common Fund to advance the infrastructure and processes by which AI can usher in the future of biomedical research. Top among the program’s goals are the generation of data sets that are appropriately set up for AI applications and the development of best practices for the application of ML and AI.
“We are building standards across broad segments of the biomedical domain to make data sets interpretable for computerized learning,” says Alex Wagner, PhD, principal investigator in the Institute for Genomic Medicine at Nationwide Children’s and a co-lead of the Bridge2AI coordination center standards core. His efforts involve development of standards to structure and annotate data sets so that, from institution to institution, certain key structures or elements remain the same and can be used by ML or AI to navigate and interpret the data.
“It’s an enormous undertaking to invest in AI from the ground up, not just in the data standards we are working on in the Global Alliance for Genomics and Health,” Dr. Wagner says. “Bridge2AI also has experts working to create foundations for AI’s ethical use, the ability to identify bias in data sets, accessibility for research, and much more. I think it bodes very well for our ability to mine these data for insightful, AI-based discovery down the road.”
Even seemingly basic applications of AI require carefully designed infrastructure and data features. And of course, they must be highly accurate and fit for purpose in order to be ethical and useful.
“When we implement AI in health care settings, we have to be extremely diligent,” says Dr. Bartlett, who has painstakingly worked to design and deploy Nationwide Children’s electronic health record (EHR) ML program.
“We need to know the weaknesses up front, watch it at every step, and build in complete transparency. Even after we have a model that we think is good enough, we implement it in the background and monitor it another 6 months to make sure it does what we want it to do.”
Only after thorough, prospective trial periods does his team release ML-based features in the EHR system. Examples of successful efforts already in practice include early prediction of sepsis, which tripled the average number of days between sepsis-related emergent transfers to the pediatric intensive care unit, and automation of predictive assessments for cardiac arrest, which matched predictive accuracy of a manual early warning tool 2 hours before a cardiac event.
These improvements, published in Pediatric Quality & Safety, are in good company; ML has also improved prediction of families at high risk for no-shows in a neurology clinic (published in the Journal of Child Neurology) and dramatically reduced in-hospital deterioration events at Nationwide Children’s (published in Pediatric Critical Care Medicine).
These applications are just the tip of the iceberg, though. Drs. Trask, Bartlett and Ray are also collaborating on work that could hit the clinic relatively soon: ML-based analysis of blood flow imaging to predict fetal growth restriction (FGR) before symptoms emerge.
“In prenatal ultrasounds, clinicians already look at blood flow through the umbilical cord,” explains Dr. Trask, who has joined forces with Mark Santillan, MD, PhD, an obstetrician at the University of Iowa with about 63,000 ultrasound files. “If by clicking a button during a routine ultrasound an obstetrician can find out whether this pregnancy is at heightened risk for complications due to FGR, that’s a no-brainer addition to practice. It would immediately change that pregnancy’s management.”
Other potential applications to clinical practice may also become available sooner rather than later.
“ML models are already helping us classify tumors from epigenomic assays, but soon it could feasibly offer decision support for variant interpretation as well,” Dr. Wagner suggests. “It could predict how patients will respond to therapeutics and prompt data requests to help improve its prognostic ability, perhaps by suggesting what other test results it needs to be more useful for a patient.”
This type of interactive, personalized medicine comes at a price, of course, and has some specific hurdles to overcome before its widespread implementation in the world of pediatrics compared to adult medicine.

A Child-Focused Approach To AI
Three key factors distinguish AI in pediatrics from its use elsewhere in health care: reconsenting as children age so that data may continue to be used ethically; aging and its implications for ML modeling accuracy; and the complexity of source data.
Consent
When working with pediatric data that was obtained via parental consent, it is important to note that approval for use of their data is re-obtained when children reach the age of consent. This potentially limits its use — or at the very least requires strict monitoring of consent status — over time.
For applications of ML in EHRs, long-term access to files will also dictate how well programs can train language processors and track how kids’ health indicators change with age. The concept of change over time is critical for a variety of pediatric-specific conditions and opens another, more nuanced area of difference from adults: the importance of growth.
Growth and Aging
“For kids, three years is the difference between no head control at all and running all over the place, whereas adult health is usually fairly stable within that same amount of time,” says Dr. Bartlett.
This growth factor adds a layer of complexity to any analysis done in children: how does their data change as they age, and what does that mean for the models being developed?
Data Complexity
These challenges are compounded by extra inputs into medical records and more frequent changes in providers. In most adult records, for instance, files include notes only from the patient and the clinician. With children, there may be notes from parents or other caregivers clinicians, the children themselves, numerous subspecialists and even teachers or social workers.
“When we merge all of these data sources together, it is harder to come up with accurate predictions,” says Dr. Sezgin, who specializes in analyzing the health care applications of AI and recently published in The Lancet Child & Adolescent Health on its ethical use in pediatrics. “Many applications of ML and AI employ models that were trained using publicly available adult data sets, since pediatric data sets are less accessible due to higher standards for privacy and security. These higher thresholds for protection are appropriate, but they mean that translating those models for accurate predictions in pediatric care is challenging.”
As children age, they frequently transition among facilities and, eventually, to adult providers. This can result in gaps in records or a large volume of notes to examine for insights. The result of all of these factors is a dramatic increase in data diversity and availability challenges, as well as much greater burden for NLP applications, making it difficult to tease out what weight to give the different inputs and what to do if certain inputs are missing.
These electrocardiogram (ECG) and Doppler echocardiogram images were collected and analyzed as part of Dr. Trask’s collaborative and ongoing ML-based analysis of blood flow in order to predict microvascular disease. Details on the study’s findings were published in Scientific Reports.
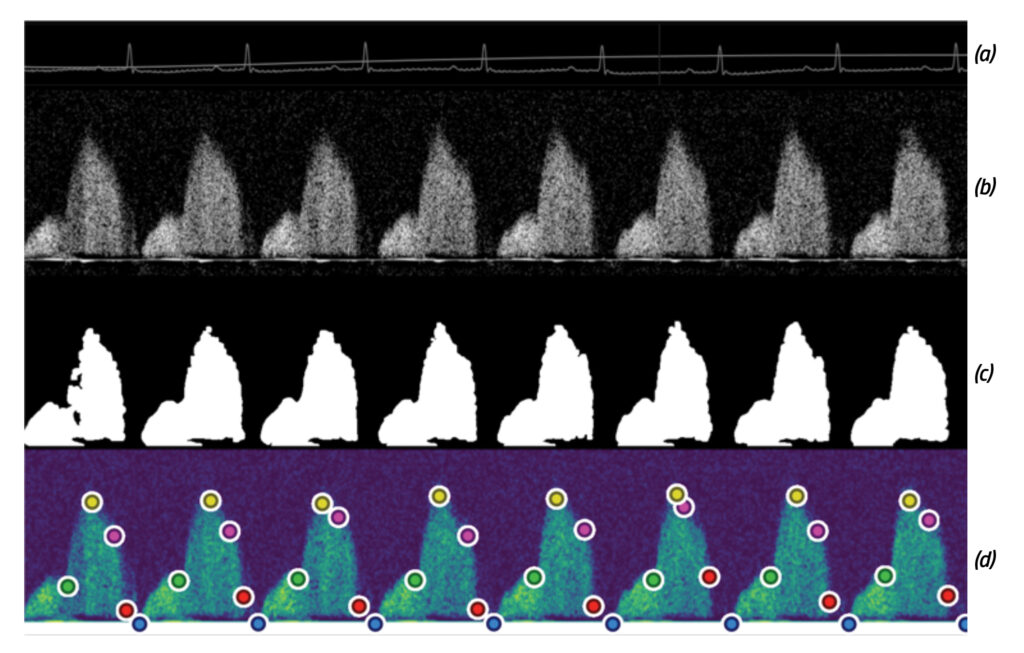
(a) ECG tracing output from mouse studies (b) Raw Doppler echocardiogram output of mouse coronary blood flow (c) Automated Doppler envelope extraction by the team’s software program (d) Inflection points of the Doppler that the automated ML program uses to extract data regarding the “envelope,” or mountain-shaped patterns, indicating blood flow
A Productive, Ethical and Equitable Future For AI
Regardless of the data source, Dr. Sezgin urges caution.
“Using AI is like teaching a little kid: you need to show them how to behave correctly, like stopping at a red light,” he says. “If you don’t train them properly, it could be dangerous for the child and everyone else. Likewise, these tools have great potential for pediatric settings — if they are employed with a careful team to guide them in the right direction.”
This guidance involves placement of safety and privacy parameters on accessible data as well as understanding the inherent limits of AI. After all, it can only be as accurate as the data it has on hand.
Just as prediction models trained by adult data sets fall short for predictions in pediatrics without new data to improve the model, data sets with limited information about minority populations have been shown to be less effective at predictions for those populations. Unfortunately, pediatrics faces the same challenge as adult medicine in this regard: inequities in care access and research participation result in fewer data sets available for minorities.
“We are failing to serve vulnerable populations in the health system, and this problem doesn’t go away when we apply AI downstream,” says Dr. Sezgin. “These technologies will only reflect the quality of the data they receive — they won’t serve everyone unless the health care system does a better job of creating fair, equitable, representative medical data first.”
That said, Dr. Sezgin does believe AI can help improve the health system itself if applied strategically. His Chatbot for Social Needs project, funded by the Health Resources and Services Administration, uses conversational AI to address families’ social needs, able to contribute to medical records with patients’ self-reported health information and communicate with providers. The project aims to address social determinants of health, improve shared clinical decision-making and advance preventive medicine.
While experts in biomedical ML and AI projects temper their enthusiasm with caution, one thing is consistent across the board: an expectation that computer-based algorithms will revolutionize the way clinicians spend their work day, the way that pediatric patients experience their care, and the way improved outcomes and new discoveries are achieved.
At the end of the day, clinicians need to understand what factors the model is using to make its predictions. It can’t be a black box to them, or physicians won’t be able to rely on it for their own decision-making.”
– Aaron Trask, PhD, FAHA, principal investigator in the Center for Cardiovascular Research at Nationwide Children’s Hospital
At Nationwide Children’s, the commitment to meeting challenges and surpassing expectations in the AI frontier is evidenced by the appointment of Peter White, PhD, as the inaugural chief data science officer at AWRI.
As a member of the AWRI senior leadership team, Dr. White will be responsible for building and executing a comprehensive data science strategy across AWRI, including the integration and analysis of disparate big data sources such as genomic and electronic health record data as well as using artificial intelligence and machine learning techniques to derive insights for the diagnosis and treatment of pediatric diseases. He will oversee a team of data scientists, software developers, cloud engineers, data architects, analysts and other professionals to support these efforts.
“In his new role as CDSO, he will work to empower our research community with cutting-edge data science capabilities and promote a culture that values making data accessible, removing barriers to access, and promoting transparency, collaboration and information sharing,” says Dennis Durbin, MD, MSCE, president of AWRI. “His leadership in biomedical data science will substantially support Nationwide Children’s mission as a leader in pediatric health care innovation.”
As the infrastructure and data sources fall into place, the time is right for well-informed, collaborative experts to begin harnessing the potential of these tremendous resources, while keeping pediatric specific considerations in mind. With patience and due diligence, it’s not a matter of whether these tools will transform the practice of medicine, but when.
This feature was published in the Spring/Summer 2023 issue. Download the full issue.
References:
- Bartlett C, Bossenbroek J, Ueyama Y, McCallinhart P, Peters OA, Santillan DA, Santillan MK, Trask AJ. Ray WC. Invasive or more direct measurements can provide an objective early-stopping ceiling for training deep neural networks on non-invasive or less-direct biomedical data. Springer Nature Computer Science. In press.
- Boch S, Sezgin E, Lin Linwood S. Ethical artificial intelligence in paediatrics. Lancet Child & Adolescent Health. 2022 Dec;6(12):833-835.
- Bossenbroek J, Ueyama Y, McCallinhart PE, Bartlett CW, Ray WC, Trask AJ. Improvement of automated analysis of coronary Doppler echocardiograms. Scientific Reports. 2022 May 6;12(1):7490.
- Gorham TJ, Rust S, Rust L, Kuehn S, Yang J, Lin JS, Hoffman J, Huang Y, Lin S, McClead R, Brilli R, Bode R, Maa T. The Vitals Risk Index-retrospective performance analysis of an automated and objective pediatric early warning system. Pediatric Quality & Safety. 2020 Mar 20;5(2):e271.
- Peng J, Patel AD, Burch M, Rossiter S, Parker W, Rust S. Predicting patient no-shows in an academic pediatric neurology clinic. Journal of Child Neurology. 2022 Jun;37(7):582-588. Nuss KE, Kunar JS, Ahrens EA. Plan-Do-Study-Act methodology: refining an inpatient pediatric sepsis screening process. Pediatric Quality & Safety. 2020 Sep 2;5(5):e338.
- Sezgin E, Oiler B, Abbott B, Noritz G, Huang Y. “Hey Siri, help me take care of my child”: A feasibility study with caregivers of children with special healthcare needs using voice interaction and automatic speech recognition in remote care management. Frontiers in Public Health. 2022 Mar 3;10:849322.
Image credits: Adobe Stock (header); Nationwide Children’s (portraits)
About the author

Katherine (Katie) Brind’Amour is a freelance medical and health science writer based in Pennsylvania. She has written about nearly every therapeutic area for patients, doctors and the general public. Dr. Brind’Amour specializes in health literacy and patient education. She completed her BS and MS degrees in Biology at Arizona State University and her PhD in Health Services Management and Policy at The Ohio State University. She is a Certified Health Education Specialist and is interested in health promotion via health programs and the communication of medical information.
- Katie Brind'Amour, PhD, MS, CHEShttps://pediatricsnationwide.org/author/katie-brindamour-phd-ms-ches/

- Katie Brind'Amour, PhD, MS, CHEShttps://pediatricsnationwide.org/author/katie-brindamour-phd-ms-ches/
- Katie Brind'Amour, PhD, MS, CHEShttps://pediatricsnationwide.org/author/katie-brindamour-phd-ms-ches/
- Katie Brind'Amour, PhD, MS, CHEShttps://pediatricsnationwide.org/author/katie-brindamour-phd-ms-ches/


