
THRIVING After Severe Bronchopulmonary Dysplasia
THRIVING After Severe Bronchopulmonary Dysplasia https://pediatricsnationwide.org/wp-content/uploads/2021/02/BPD-2-1024x731.jpg 1024 731 Abbie Miller https://pediatricsnationwide.org/wp-content/uploads/2023/05/051023BT016-Abbie-Crop.jpg
Meet Willow. She was born via emergency C-section at just 22 weeks. Doctors at the delivering hospital told Willow’s mom Cortney that her baby’s chances of survival were low. But after a long journey through the newborn intensive care unit (NICU) at Nationwide Children’s Hospital, Willow is a vivacious 4-year-old looking forward to starting kindergarten in the fall.
“Willow’s biggest obstacle during her NICU stay was her lungs, due to developing severe bronchopulmonary dysplasia,” says Cortney.
Willow isn’t alone. Each year, 10,000 to 15,000 babies born preterm are diagnosed with severe BPD, according to the National Institutes of Health. However, not everyone’s story has the same happy ending.
Babies with severe BPD are at high risk for mortality and morbidities. In fact, according to Edward Shepherd, MD, section chief of Neonatology at Nationwide Children’s, for preterm infants, in those first few days and weeks BPD and death are competing outcomes — that is, survival often comes with BPD.
“At 22 to 32 weeks gestation, babies’ lungs are underdeveloped,” he says. “Our first task is to keep them alive. The second task is to minimize the damage to the developing lungs.”
Neurodevelopmental delays, including hearing and vision impairment, cerebral palsy or delays on Bayley’s scales (developmental tests), are a common outcome for the babies with severe BPD who survive.
Willow developed what Dr. Shepherd calls “super severe BPD.” She spent 4.5 months on a ventilator before graduating to CPAP. After two months of CPAP, she graduated to a nasal cannula. Finally, at age 3 she stopped needing any oxygen support.
PREVENTING NEURODEVELOPMENTAL CONSEQUENCES OF BPD
All babies born preterm are at risk for neurodevelopmental delays and impairments. Those who develop BPD are at even higher risk.
“Historically, the medical community thought that the neurodevelopmental problems associated with BPD were caused by the lung disease,” says Dr. Shepherd, who is also associate professor of Clinical Pediatrics at The Ohio State University College of Medicine. “But other lung diseases don’t cause neurodevelopmental delays. So, we needed to look at how we’re treating the lung disease and how that could be affecting the brain.”
Traditionally, doctors have treated BPD in the same way that they tried to prevent it — by minimizing time on the vent, keeping babies sedated and using intravenous (IV) nutrition.
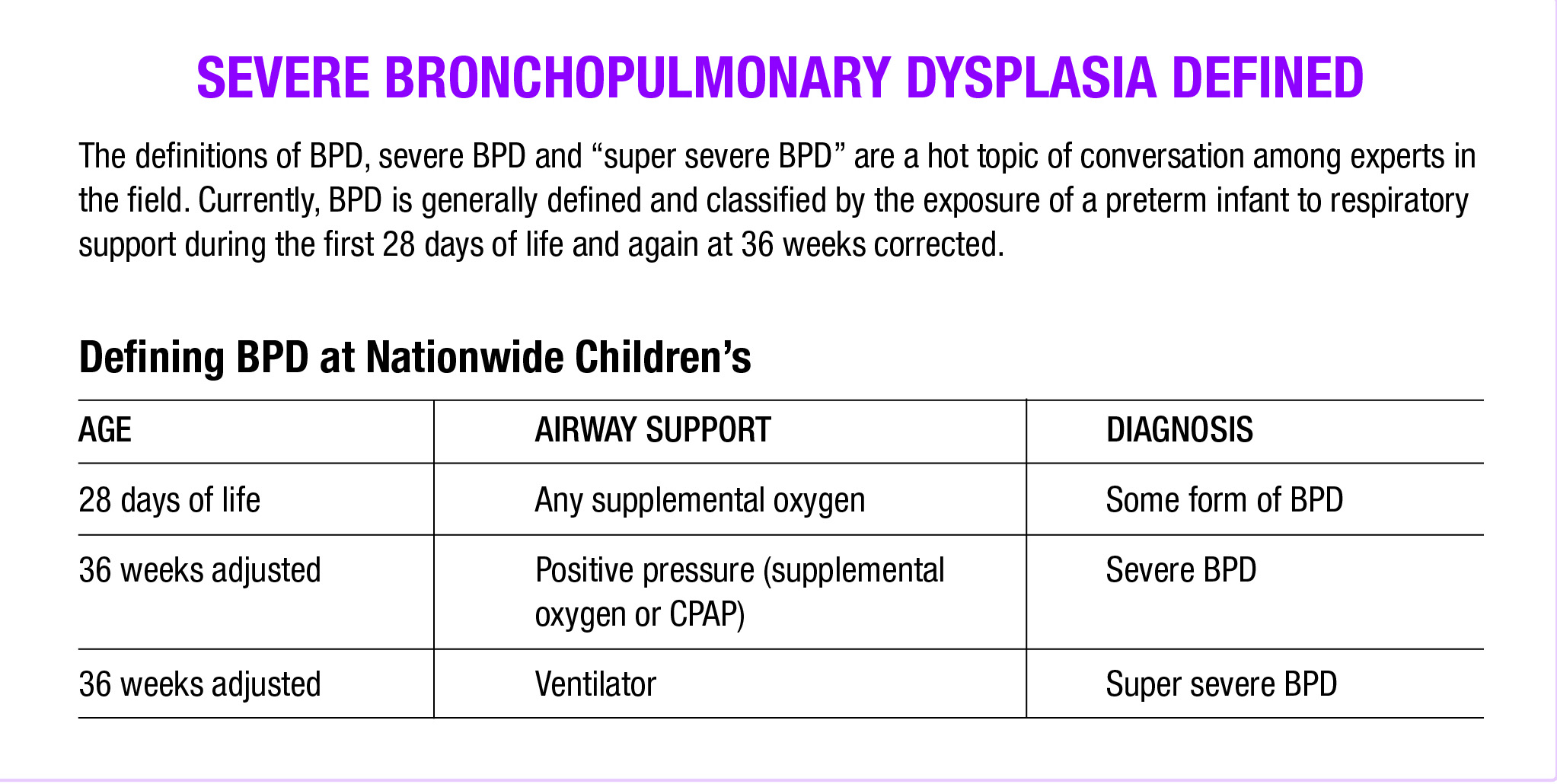
“But 12 weeks later, when the baby is 36 weeks adjusted and officially diagnosed with severe BPD, we’re still doing that,” says Dr. Shepherd. “We need to shift away from treating it like an acute disease.”
Despite the prevalence of BPD among preterm infants, there isn’t a lot of consensus on the true cause of the disease or the best way to treat the disease after 36 weeks adjusted age.
“Once they get to 36 weeks and still need significant respiratory support, they have severe BPD. The strategies used to prevent BPD are no longer an effective approach to treatment,” says Stephen Messier, MD, medical director of Neonatology at Sanford Children’s Hospital Sioux Falls. “It takes a different way of thinking – and the acceptance that we’re now treating something that will take months to years to get better. Not days to weeks like most other things we treat in neonatology.”
Treating BPD as a chronic disease is the keystone to the care model used by the Comprehensive Center for Bronchopulmonary Dysplasia (CCBPD) at Nationwide Children’s.
“If a baby has 12 weeks of accumulated disease, they’re not going to get better today. Or tomorrow,” says Dr. Shepherd. “We have to adjust the treatment and our expectations and move at the pace of the baby. And in doing so, we improve outcomes and actually shorten average lengths of stay.”
Change Vent Settings
Have you ever held your breath for too long? It’s an uncomfortable feeling. For babies who aren’t properly oxygenated, that feeling of being “air hungry” is a powerful stress on the body.
Using different vent settings can reduce this stress. Once BPD is established, Dr. Shepherd’s team moves to a management strategy for severe BPD. [Download the vent settings used by the Nationwide Children’s team.]
“We go from low tidal volumes, short inspiratory times and high rates to high tidal volumes, longer inspiratory times and low rates,” says Dr. Shepherd. “This shift is a different paradigm and can make some people uncomfortable. But we’re continuing to show that this approach works.”
In other words, they go from breathing fast, small breaths to breathing slower, deeper breaths.
The goal for respiratory support in the chronic care model is avoiding air hunger, keeping the babies “pink and comfortable” at all times.
Create a Joyful NICU
When you walk into the BPD Unit of Nationwide Children’s, it’s easy to forget you are in a NICU. Infants are sitting on parents’ laps, participating in music therapy while intubated or attached to a CPAP machine. In another room, a baby sits in a baby seat on the floor, CPAP tubes attaching her to the machine that helps her breath, while she plays with an array of brightly colored toys. Two doors down, a set of twins sharing a room are in their cribs, settling down for a nap, while their older sibling reads them a story.
“We are indeed a highly-skilled level 4 intensive care center,” says Dr. Shepherd. “But we apply a model of care for BPD in which we are minimizing pain and noxious stimuli and maximizing joy.”
As the only center of its kind, the BPD Unit becomes home to infants with severe BPD from around the country as they wait for their lungs to get strong enough for the outside world. The BPD Unit opened in 2005, but the team had started applying the model — including altered vent settings — as much as possible before that.
“We treat them developmentally appropriately — not waking them up. Minimizing pain and IVs. Letting parents hold them as much as they want 24/7. And relying more on physical exams and assessments to minimize blood draws and tests,” Dr. Shepherd says.
Maximizing fun can be difficult to do in the NICU, but with the support of the nursing staff, and by enlisting many different therapists — including music and occupational therapists — working with parents and educating the team, it can be done.

Michelle Hull, a member of the Early Childhood Development Team, working with a patient on the BPD Unit and her family. The Early Childhood Development Team provides individualized developmental support for patients using a play-based model. Here, Michelle is coaching parents during a bedside play session focusing on communication and social skills.
Participate in Research
Babies in the BPD Unit have access to all the neurodevelopmental protocols and research offered in the NICU at large. Nathalie Maitre, MD, PhD, is a neonatologist and developmental specialist at Nationwide Children’s. And she’s the leader of many research protocols, including the Baby Brain Optimization Project (BBOP), aimed at supporting healthy neurodevelopment in the NICU.
“The NICU environment is very different from the home environment,” she says. “The stimuli that a baby is exposed to in the NICU can be detrimental to the developing brain. And certain protective stimuli — such as mother’s voice and touch – are sorely missing.”
By including babies with BPD in the neurodevelopmental protocols and interventions, their brain development can be further optimized, she says.
CHANGING [MORE THAN] NEURODEVELOPMENTAL OUTCOMES
“We applied this chronic care model relentlessly over time. We thought that it would improve neurodevelopmental outcomes — and it did. But it also did so much more. Our survival rates also increased to 99% for severe BPD. Nationally, survival rates are 80-90%,” says Dr. Shepherd.
According to Dr. Shepherd, patients in the BPD Unit at Nationwide Children’s have about 10-15% risk of neurodevelopmental impairment compared to 40-50% in the national sample.
Recently, the Nationwide Children’s team published the results of a retrospective observational study following 151 consecutive patients with moderate to severe BPD who were treated in the BPD Unit at Nationwide Children’s. The study, published in The Journal of Pediatrics, includes data that support the concept of a comprehensive, neurodevelopmentally oriented approach.
According to the study, patients treated with this approach had better neurodevelopmental outcomes than previously reported cohorts. Additionally, the only two factors that were significantly associated with neurodevelopmental impairment at 24 months of age were lower birth weight and longer hospital stays.
“Shorter length of stay is one of the benefits to the comprehensive, chronic care approach,” says Dr. Shepherd. “This study confirms that we’re on the right track.”
As great as those results are, they are only for a single center. In order to have an even better chance at improving outcomes for babies with BPD, large, multicenter studies are needed.
“That’s exactly why we started the BPD Collaborative,” says Leif Nelin, MD, division chief of Neonatology at Nationwide Children’s and chair of the BPD Collaborative.
The BPD Collaborative was formed in 2012 to fill knowledge gaps around the care of infants with BPD by sharing data, conducting research and developing quality improvement initiatives. It started with six other centers and has more than doubled in size to include Nationwide Children’s and 17 other institutions.
“When we started, we didn’t have any funding, so we were all doing this on our own. We began having regular meetings and teleconferences and a few studies,” says Dr. Nelin, who is also professor of Pediatrics at OSUCM. “But as funding came, we began to conduct more research and submit more publications.”
In 2017 the BPD Collaborative published the “manual” on how to care for these infants, establishing the first consensus guidelines on the condition. Since then, their work has continued.
“One of the biggest challenges to BPD research is that each institution does things a little (or a lot) differently,” says Dr. Nelin. “There’s no blinded clinical trial to compare prevention and treatment approaches, so we’re focused on comparative effectiveness research.”
Part of this research is aided by a large database, supported by the BPD Collaborative member institutions. The database enables large datasets to be gathered, allowing for broader studies.
The Collaborative is also taking aim at a deeply phenotyped and genotyped study of patients with BPD by submitting a grant proposal to the NIH. The study will facilitate understanding of the causes of BPD and best treatments, by looking for genetic variations that may better predict outcomes in a large — 600 patient — cohort of infants with BPD.
“BPD is an interesting disease,” says Dr. Nelin. “If you ask a neonatal practitioner, they can tell you what BPD is, but when you ask them to define it, it’s really hard to do. We are really excited to dig deeper into ways to define the condition that are more predictive of outcomes. And hopefully, that will lead to precise medicine approaches to BPD treatment.”
LIFE AFTER THE NICU
Willow was able to finally go home after 236 days in the NICU. She came home using oxygen on a nasal cannula and a G-tube to assist with feedings. Her care plan included weekly physical therapy and months of follow-ups in the BPD Clinic.
The BPD Clinic at Nationwide Children’s operates as a “medical home model.” That is, BPD experts work closely with the child’s primary care physician to oversee the care and progress of the whole patient.
The model is fundamentally interdisciplinary.
“Interdisciplinary care teams are extremely important to support all the needs of the patient with BPD and their families,” says Susan Lynch, MD, medical director of the BPD Clinic at Nationwide Children’s. “From nutrition experts, social workers, developmental therapists and respiratory therapists to nurses, physicians and nurse practitioners — all members play a vital role in the holistic care of the infant and child with BPD.”
And the team is available 24/7.
“It is incredibly important for families of patients with BPD to be able to have access to the care team to ask questions about changes in their baby,” says Dr. Lynch, who is also an associate professor of Pediatrics at OSUCOM. “The BPD Clinic provides this access no matter the day or time. We also encourage primary care providers to work closely with the family and the BPD team to help address the family’s questions and evaluate the baby during times of change if they live far from Columbus.”
By providing round-the-clock access, the BPD team can address concerns early and often keep little ones out of the Emergency Department by seeing them in the BPD clinic, adds Dr. Lynch. It also provides the needed support to help families build confidence in their child’s care, successfully taking their child outside the hospital setting and gaining a deeper understanding of their child’s medical needs over the first three years of life.
After the implementation of the BPD program and the initiation of the BPD Clinic in 2004, one month readmission rates of patients with BPD decreased from 29% to 5%.
BPD NEURODEVELOPMENTAL FOLLOW-UP CLINIC
NICU follow-up care in the BPD clinic is divided into two subclinics: one focusing on a child’s medical needs and the other focusing on their developmental needs.
“We found that for many families, having both medical and developmental combined into the same clinic visit was just overwhelming,” says Dr. Maitre, director of NICU Follow-up Programs. “To first discuss whether or not your child was getting enough oxygen and move right on to whether he or she was meeting developmental milestones is a lot for parents to take in and process.”
By splitting the follow-up care into two clinic visits, the teams are able to spend more time with the families, give them digestible amounts of information and address their questions.
“We focus a lot on minimizing neurodevelopmental impairments in the NICU and improving neurodevelopmental outcomes,” says Dr. Maitre. “It’s important to remember that a child with a neurodevelopmental delay is not a failure, however. We give that family a good outcome by empowering them to handle whatever comes their way. An empowered family is a good outcome.”
A BRIDGE FROM BPD CLINIC TO PULMONARY MEDICINE
Once children age out of the BPD clinic — around age 3 — they are followed by a pulmonologist.
“But not just any pulmonologist,” says Dr. Maitre.
Daniel Malleske, MD, MS, is board certified in internal medicine, pediatrics and neonatology. And he’s completing a fellowship in pulmonary medicine. For patients with BPD at Nationwide Children’s, he’s the bridge between the BPD clinic and lifelong pulmonary care.
“I think that the field could really benefit from doctors who are interested in following these patients through childhood and into adulthood — and conducting research and intervening wherever possible,” says Dr. Malleske. “I decided to be one of those doctors.”
Survivors of prematurity — with or without BPD — are at an increased risk for pulmonary complications, such as greater airway reactivity, greater air trapping and exercise limitations, in adulthood. For those with BPD, the risk is especially high.
As children with BPD age, they can present with asthma-like symptoms. In fact, those symptoms are primarily managed with asthma medications.
“We really don’t know the natural history of lung function of patients with BPD into later adulthood. Most are in their 40s at the oldest,” says Dr. Malleske. “We’re seeing examples of emphysema, or chronic obstructive pulmonary disease, in patients who were born preterm or who had BPD. They are developing COPD at earlier ages and without the common lifestyle factors.”
Once he finishes his fellowship, Dr. Malleske says he is looking forward to resuming research in long-term airway development and pulmonary function in the surviving BPD population.
IMPROVING CARE EVERYWHERE FOR BABIES WITH BPD
As many as half of the patients at any one time in the BPD Unit may be from outside the Nationwide Children’s region. And almost all of those had a do not resuscitate order (DNR) at their previous institution.
“Parents find us online and call us asking for help. Increasingly providers are calling, too,” says Melinda Ingram, CPNP-PC. “In many cases, we can work with a willing provider at an outside NICU to help improve things for the baby at their home hospital, but sometimes transfer is the best option.”
“We begin talking with the providers, and sharing what we would do,” says Dr. Nelin. “They implement some (maybe not all) of the things, and the baby ends up improving and being more stable at time of transfer. This gets that institution thinking about the next patient, and how they can adopt some of the things we do.”
One example of how a transfer case became a lasting relationship with another institution, is a case from South Dakota nine years ago. A patient for whom the team at Sanford Children’s Hospital had done all they could was ultimately transferred to Nationwide Children’s at the parents’ request. The baby survived and is doing well to this day, says Dr. Nelin.
Dr. Shepherd shared the chronic care model used in the BPD Unit at Nationwide Children’s with the team at Sanford as he’s done for other hospitals around the country. And since then, the two institutions have continued to work together to improve care for infants with BPD. “We still transport the occasional infant to Nationwide Children’s,” says Dr. Messier. “But we can keep a lot more of them closer to home now.”
“No baby should die from BPD or have a decreased quality of life from the disease,” says Dr. Shepherd. “We’re excited to share what we’re learning, and we look forward to learning even more together. That’s why we have the BPD Collaborative. Why we publish. And why we consult with other institutions openly.”
This story appeared in the 2020 Spring/Summer print issue. Download the full issue.
References:
- Abman SH, Collaco JM, Shepherd EG, Keszler M, Cuevas-Guaman M, Welty SE, Truog WE, McGrath-Morrow SA, Moore PE, Rhein LM, Kirpalani H, Zhang H, Gratny LL, Lynch SK, Curtiss J, Stonestreet BS, McKinney RL, Dysart KC, Gien J, Baker CD, Donohue PK, Austin E, Fike C, Nelin LD. Interdisciplinary care of children with severe bronchopulmonary dysplasia. Journal of Pediatrics. 2017 Feb; 181:12-28.
- Nelin LD, Bhandari V. How to decrease bronchopulmonary dysplasia in your neonatal intensive care unit today and “tomorrow”. F1000Res. 2017;6:539.
- Malleske DT, Chorna O, Maitre NL. Pulmonary sequelae and functional limitations in children and adults with bronchopulmonary dysplasia. Paediatric Respiratory Reviews. 2018;26:55–59.
- Bauer SE, Schneider L, Lynch SK, Malleske DT, Shepherd EG, Nelin LD. Factors associated with neurodevelopmental impairment in bronchopulmonary dysplasia. Journal of Pediatrics. 2020;218:22–27.e2.
Image credits: Nationwide Children’s
About the author

Abbie (Roth) Miller, MS, MWC, is a passionate communicator of science. As the manager of medical and science content at Nationwide Children’s Hospital, she shares stories about innovative research and discovery with audiences ranging from parents to preeminent researchers and leaders. She is a Medical Writer Certified®, credentialed by the American Medical Writers Association, and received her masters of science in Health Communication from Boston University.
- Abbie Millerhttps://pediatricsnationwide.org/author/abbie-miller/

- Abbie Millerhttps://pediatricsnationwide.org/author/abbie-miller/
- Abbie Millerhttps://pediatricsnationwide.org/author/abbie-miller/
- Abbie Millerhttps://pediatricsnationwide.org/author/abbie-miller/


