
Clinical Genomics: From Research to Reality
Clinical Genomics: From Research to Reality https://pediatricsnationwide.org/wp-content/uploads/2025/03/for-web-Cover-Concept_FINAL-1024x716.jpg 1024 716 Abbie Miller https://pediatricsnationwide.org/wp-content/uploads/2023/05/051023BT016-Abbie-Crop.jpg
Without genomic sequencing, many genetic diseases would never be diagnosed.
Genomic testing — whole exome or whole genome sequencing — is vital to reducing the diagnostic odyssey for children with rare, undiagnosed disease. But is genetic analysis only useful in these cases?
Experts across the country have long suggested that genomic testing can be even more useful as a frontline test. An evidence-based clinical guideline from the American College of Medical Genetics and Genomics, led by Kandamurugu Manickam, MD, MPH, FACMG, clinical geneticist and genomicist at Nationwide Children’s Hospital, highlights the higher diagnostic yield of genomic testing compared to standard genetic testing, especially for patients with congenital anomalies, developmental delay or intellectual disability. However, issues of cost, scaling and proving the return on investment have stood in the way of making it a reality.
The Human Genome Project was a watershed moment in scientific history when it was completed in 2003. It took 15 years and about $3 billion to accomplish. By 2015, using next generation sequencing (NGS) that same genome took about one day and cost around $2,000. Since then, the process to generate human genome sequencing data has gotten even faster.
MOVING TO THE CLINIC
One of the early, large-scale studies to establish the potential benefits of genomic sequencing for newborns is the BabySeq Project. This ambitious venture sequences both well babies and those admitted to neonatal intensive care units.
Early data published by the BabySeq Project showed that actionable information was found for both seemingly well and more obviously sick infants. Sequencing provided a benefit to both groups, supporting the movement to incorporate genomic testing more broadly in health care.
“The broader application of genomics for both sick and well children represents the next era in genetic and genomic medicine. It is our goal as an institution to lead the way into this new era,” says Beth Kozel, MD, PhD, chief of the Division of Genetics and Genomic Medicine and the director of Constitutional Genomics Translational Research in the Steve and Cindy Rasmussen Institute for Genomic Medicine at Nationwide Children’s.
Dr. Kozel’s vision for the future is one in which genomic information becomes part of the “everyday medical and health care experience.” By utilizing rapid genome sequencing (rGS), which can return results as fast as three days, the clinical and laboratory teams at Nationwide Children’s are already making strides on one important goal: the fastest diagnoses for the sickest patients.
RAPID GENOMES: IMPACT IN ACTION
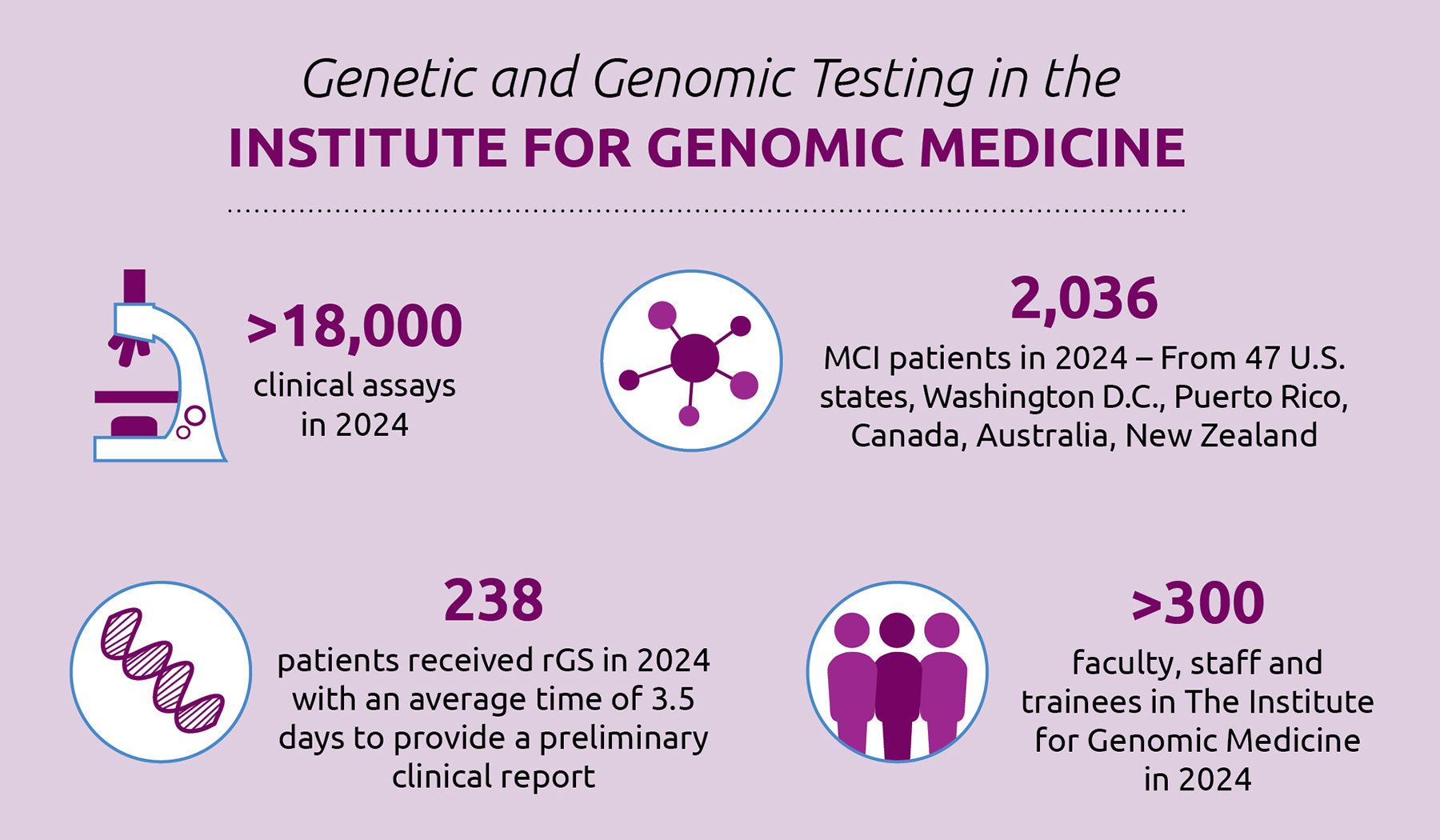
On January 8, 2024, clinical rGS rolled out hospital- wide at Nationwide Children’s main campus, and uptake has been higher than expected. Between launch and December 31, 2024, the team has completed more than 220 rapid genome patient samples and nearly 350 rapid parent samples, which are used to act as a reference when analyzing patient sequences.
The development of clinical rGS was a significant undertaking and major accomplishment for the Clinical Laboratory within the Institute for Genomic Medicine. Led by Section Chief Catherine Cottrell, PhD, FACMG, a team of highly skilled clinical directors, variant scientists/analysts, and laboratory genetic counselors partnered with Institute for Genomic Medicine managers and supervisors, technologists, technology development specialists, and bioinformaticians to transition this assay from a research test to a clinical offering.
“Working with clinicians who have been with us every step of the way enables us to bring the most impactful genomic tests to the clinic,” Dr. Cottrell says. “This is possible because of the organization’s culture. We’re less siloed than a lot of organizations, and that makes us innovative and nimble.”
This clinical testing was developed out of a translational research protocol within the Institute for Genomic Medicine, which was led by Bimal Chaudhari, MD, MPH, a neonatologist, medical geneticist and translational informaticist at Nationwide Children’s. Knowledge gained during the research protocol was crucial in honing testing workflows and streamlining analysis. This research experience shaped the transition into a clinical assay and enabled the direct return of genomic results to the patient care team for clinical decision making.
“Remarkably, our teams were able to provide a diagnosis for 28% of rapid cases in 2024,” says Dr. Kozel. “This shows that we are testing the right patients and providing life-changing information, hopefully in time for it to impact care and improve outcomes.”
Even when testing doesn’t find a diagnosis, it can still aid medical decision making — sometimes knowing that a certain diagnosis is not present can be as valuable to the care plan as knowing that it is.


EARLY SUCCESS IN THE NICU
One of the earliest successes is the implementation of rapid genome sequencing in the neonatal intensive care unit (NICU). Historically, about a quarter of neonates who receive early life genetic testing do not get their results back until after discharge. While the information from those tests may help direct their care long term, often the delay represents a missed opportunity for the genomic information to impact care immediately in the NICU.
The Nationwide Children’s rGS program aims to change that.
“About 50% of genomic tests happen in the first week in the NICU — this is when it is most cost effective because it has the highest potential to impact care,” explains Dr. Chaudhari.
For example, genomic results could influence when or if to do surgery, not just in the NICU but in any ICU situation. However, in these high-acuity areas, decisions can’t wait indefinitely.
“That’s why we need to test as early as possible when there’s an indication there could be benefit to having the genome data,” says Dr. Chaudhari.
But how do you know who would be most likely to benefit outside of carefully selected clinical trial populations? When is the right time to order testing? Dr. Chaudhari and his colleagues are actively trying to find out when testing is most likely to offer beneficial outcomes. They recently completed a clinical pathway to support physician decision making in the area.
“It really boils down to two questions,” says Dr. Chaudhari. “Is the patient sick? Do you know why this is happening?”
If a patient is sick and the treating clinician doesn’t know why, a robust body of evidence suggests moving expeditiously to rGS can change the outcome for that child.
Even if a clinician thinks they know why a child is sick, should they consider getting a genomic test? If a newborn is sick enough to be in a Level IV NICU, is a genomic test warranted?
Currently, no research answers these questions, but a collaborative effort between the Neonatology and Medical Genetics teams is in process. Debates in terms of cost, potential benefit, bandwidth of teams, and availability of genetic counselors all factor into just how widespread genomics as a first-line test can become.
BEYOND THE ICU
rGS could apply in some acute care settings, as well, suggests Dr. Chaudhari. Finding those use cases is an increasingly interesting challenge that he looks forward to addressing.
Because the threshold for genomic testing is higher in acute care, the number of patients who receive rGS or non-rapid sequencing in an acute care setting may be smaller than in critical care. For example, a patient who is admitted repeatedly and, as a result, misses clinic appointments where they would be receiving a genomic test may be better served by receiving genomic testing during their acute care stay. This, he suggests, would make a direct impact on the trajectory of care and outcomes for the child, especially if the reason for repeated admission turns out to be genetic.
“But, there are a finite number of genetic counselors, medical geneticists and only 24 hours in a day,” he adds. “Scaling is our next frontier.”
SETTING A NEW STANDARD FOR PRECISION MEDICINE FOR CANCER
Using genomic data to better understand individual tumors and cancer cases is another area where the impact of genomic testing in the clinical setting is clear.
The National Cancer Institute (NCI) Molecular Characterization Initiative (MCI) is a national project that aims to collect, analyze and report clinical molecular data from children with a primary cancer diagnosis. The MCI is currently enrolling cancer patients from age 0 to 25 being cared for at more than 226 Children’s Oncology Group (COG)-affiliated hospitals and clinics. The data from MCI aids the referring clinicians in choosing the best treatment for each child through precision diagnosis.
The MCI is a collaboration among the National Cancer Institute, COG and Nationwide Children’s. The Biopathology Center (BPC) at Nationwide Children’s processes and stores samples from across the country for the MCI, sending the extracted DNA and RNA for these samples to the Institute for Genomic Medicine for clinical testing. The institute then conducts three separate molecular and genomic tests on the samples, analyzes the data generated and delivers timely, clinically relevant data to the practicing oncologists. Overall, the aim is to return these results within 21 days from the receipt of samples at the BPC.
It is the largest initiative of its kind in the United States and its impact is already astounding.
At about three years in, more than 4,300 patients have received MCI testing and more than 90% of patients tested by MCI receive at least one cancer-relevant result that may help define their cancer care or determine their eligibility for a clinical trial. As the types of tumors being analyzed expands, and as the field of molecular characterization continues to evolve, the team looks forward to offering even more valuable information to clinicians as well as fueling future pediatric cancer research. In fact, for every patient receiving MCI testing, the resulting genomic and molecular data are de-identified and submitted to the Childhood Cancer Database Initiative (CCDI). The collective of clinical, genomic, molecular, pathology and outcomes data at CCDI will be accessible to pediatric cancer researchers to investigate and form new hypotheses.
“If you look at other first-world countries — specifically Germany and Australia — they’ve already done MCI type programs. And their aggregate results were so compelling that their federal governments agreed to pay for molecular profiling for all children with a cancer diagnosis,” says Elaine Mardis, PhD, co-executive director of the Institute for Genomic Medicine and Rasmussen Endowed Chair in Genomic Medicine at Nationwide Children’s. She also is a professor of Pediatrics at The Ohio State University College of Medicine and serves as the principal investigator for the MCI project.
The hope of the MCI is that a similar impact will be observed in the United States.
“In three years, we’ve analyzed more patients than the German and Australian studies combined,” says Dr. Mardis. “We are providing actionable results back to providers and informing the cancer care that these kids receive. We hope to amass such compelling data to support the impact of molecular testing that it becomes federally funded and provided for all U.S. children who are diagnosed with cancer.”
MORE THAN A DIAGNOSTIC TOOL
Dr. Kozel emphasizes the importance of thinking about genomic data beyond initial diagnostics.
As an expert in Williams syndrome, she has conducted extensive research at the National Institutes of Health using genomic data to help predict cardiovascular outcomes and to offer recommendations to improve the clinical care for children with this rare disease.
“While all children with William syndrome have the same deletion and diagnosis, they do not all have the same outcomes,” Dr. Kozel explains. “We can use genomic data to understand and predict who will be more likely to have complications during anesthesia, among other outcomes.”
Pharmacogenomics — the study of how a person’s genetic code influences their response to medications — is an area ripe for developing precision medicine-based approaches for everyone. In a world where genomic information is readily available for disease-specific medications, general anesthesia dosages and protocols and more could be tailored to the needs of the individual patient — not only promoting the best possible outcome but possibly preventing significant harm.
“Pharmacogenomics is just one example of how genomic data adds value to clinical care beyond supporting diagnosis,” Dr. Kozel says. “We’re ready to go deeper into exploring the impact genomic data can have on clinical care.”
Integration of genomic data in the electronic medical record would enable clinicians to be prompted to pursue genetic diagnostics, and, if done, that information could help them make the best recommendations for the patient’s care. They could even be alerted when new information about a patient’s genetic variants is published in the literature.
“This is the world we’re working toward,” says Dr. Kozel. “Where genomic information not only informs diagnosis but also informs routine care, providing the most beneficial impact over a lifespan.”
This article appeared in the 2025 Spring/Summer issue. Download the issue here.
The move from a research-first approach to genomic testing to offer more clinically available assays was driven in part by limitations in current clinical testing offerings, as well as by the decreasing cost and turn-around time of genomic sequencing.
Each genome produces approximately 6 billion data points. How do teams in the Institute for Genomic Medicine sift through the massive quantities of data to provide clinically actionable results?
References:
- Manickam K, McClain MR, Demmer LA, Biswas S, Kearney HM, Malinowski J, Massingham LJ, Miller D, Yu TW, Hisama FM, ACGM Board of Directors. Exome and genome sequencing for pediatric patients with congenital anomalies or intellectual disability: an evidence-based clinical guideline of the American College of Medical Genetics and Genomics (ACMG). Genetic Medicine. 2021;23:2029–2037.
- The BabySeq Project. https://www.genomes2people.org/research/babyseq/publications/ Accessed February 21, 2025
Image credits: Nationwide Children’s Hospital
About the author

Abbie (Roth) Miller, MS, MWC, is a passionate communicator of science. As the manager of medical and science content at Nationwide Children’s Hospital, she shares stories about innovative research and discovery with audiences ranging from parents to preeminent researchers and leaders. She is a Medical Writer Certified®, credentialed by the American Medical Writers Association, and received her masters of science in Health Communication from Boston University.
- Abbie Millerhttps://pediatricsnationwide.org/author/abbie-miller/

- Abbie Millerhttps://pediatricsnationwide.org/author/abbie-miller/
- Abbie Millerhttps://pediatricsnationwide.org/author/abbie-miller/
- Abbie Millerhttps://pediatricsnationwide.org/author/abbie-miller/


