
Considerations for Integrating Behavioral Health and Primary Care
Considerations for Integrating Behavioral Health and Primary Care https://pediatricsnationwide.org/wp-content/themes/corpus/images/empty/thumbnail.jpg 150 150 Cody Hostutler, PhD https://pediatricsnationwide.org/wp-content/uploads/2021/03/052417ds1333-profile.jpgAs increasing numbers of pediatric patients require behavioral health care, primary care providers look to integrate behavioral health providers in their practice.
You know the story. It’s the middle of a busy Friday afternoon, you just finished up an adolescent well-visit, your hand is on the door and you hear, “Doc, one more question?” The caregiver explains that her son has seemed depressed lately and worries he may be experiencing suicidal thoughts. You assess for safety and give the family a list of referrals while your other patients grow increasingly restless. As they leave, you are left hoping that your patient is one of the 32 percent of adolescents who obtain a behavioral health within 180 days after suicidal ideation is identified in primary care. 1 If only there was someone who specializes in this kind of thing…
An integrated behavioral health provider (BHP) can support primary care providers (PCPs) in several ways including providing on-the-spot consultation, joining visits when a behavioral health concern is raised, or treating patients within the primary care center. A growing body of evidence suggests that providing behavioral health treatment improves access, outcomes and both patient and provider satisfaction.
Integrating a BHP can allow the PCP to see more patients and focus on providing services they feel more comfortable delivering and that are more lucrative. Integration also affords opportunities for increased communication between PCPs and BHPs to better coordinate treatment. Families often prefer an integrated model because they typically have the chance to meet the BHP the same day they present with a concern and follow-up can occur within the medical home, which can reduce the stigma and increase rates of follow-up.
So you think you want to integrate?
Key considerations when you begin your journey to develop an integrated model include: level of integration, range of services and range of patients.
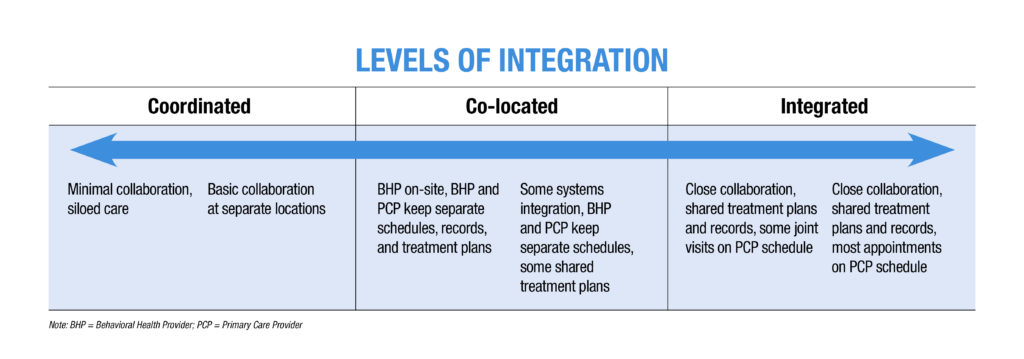
Level of Integration
Integration comes in many shapes and sizes and can range from coordinating services with a local behavioral health practice, to having a behavioral health provider conducting traditional mental health services within your practice, to having a fully integrated behavioral health provider who is primarily helping you with the patients on your schedule.
Range of Services. Do you want someone to provide intensive therapy and comprehensive psychological assessment for your most complex patients? A BHP can certainly provide this. The trade-off with this approach is that your BHP will only be able to serve a small percentage of your patients and may develop a wait-list. A BHP who provides brief, targeted intervention will be able to see more of your patients and will likely be able to maintain quick access to services, but will be somewhat limited in the scope of their practice. A BHP focused on preventive services will see a very high percentage of your patients, but will likely not have time to do much follow-up on their own schedule. Thus, the more intensive the services your BHP provides, the fewer of your patients they will be able to see and patients may have to wait longer for care. An important note is that this relationship has more to do with the complexity of services, not patients or presenting concerns.
Take a patient with emerging psychosis as an example. A BHP delivering intensive services may complete comprehensive diagnostic assessment and intensive treatment for this patient. A BHP providing brief assessment and treatment may work with the family for a few sessions to develop a plan to address a specific problem related to psychosis (e.g., school avoidance). A primarily prevention-based BHP may provide brief screening, education about what psychosis is, what the family and medical provider can expect moving forward, and relevant community resources. BHPs in every type of model will help you care for this complex patient, but the scope of their services will be different depending on level of services you would like in your clinic.
BHPs have varied levels of training and come from multiple professions (e.g., psychology, social work, licensed professional counselors, etc). In general (but not always), BHP’s with more training will be able to treat a broader range of behavioral health needs and offer a broader range of services (e.g., assessment, program evaluation, research), but may also cost more.
Range of Patients. Do you want help with a targeted problem or disease (e.g., depression, substance use, diabetes) or are you looking for someone to help you with the broad scope of patient concerns in your practice? Do you want services to be delivered to all of your patients (e.g., universal prevention model), only patients who screen positive on a specific screener, or any patient who you or the family is concerned about?
Resources
SAMHSA-HRSA Center for Integrated Health Solutions
Health Resources & Administration Health Center Program
Evolving Models of Behavioral Health Integration in Primary Care
Hunter, Christopher L., et al. Integrated Behavioral Health in Primary Care: Step-by-Step Guidance for Assessment and Intervention. 2nd edition. American Psychological Association, 2016.
Robinson P, Reiter J. Behavioral Consultation and Primary Care: A Guide to Integrating Services. 2nd edition. Springer, 2016.
Briggs RD., ed. Integrated Early Childhood Behavioral Health in Primary Care: A Guide to Implementation and Evaluation. Springer, 2016.
References:
- Chisolm DJ, Klima J, Gardner W, Kelleher KJ. Adolescent behavioral risk screening and use of health services. Administration and Policy in Mental Health and Mental Health Services Research. 2009 Nov;36(6):374-380.
- Merikangas KR, He JP, Burstein M, Swanson SA, Avenevoli S, Cui L, Benjet C, Georgiades K, Swendsen J. Lifetime prevalence of mental disorders in US adolescents: results from the National Comorbidity Survey Replication–Adolescent Supplement (NCS-A). Journal of the American Academy of Child & Adolescent Psychiatry. 2010 Oct;49(10): 980-989.
- Meadows T, Valleley R, Haack MK, Thorson R, Evans J. Physician “costs” in providing behavioral health in primary care.” Clinical Pediatrics. 2011 May;50(5): 447-455.
- Asarnow JR, Rozenman M, Wiblin J, Zelter L. Integrated medical-behavioral care compared with usual primary care for child and adolescent behavioral health: A meta-analysis. JAMA Pediatrics. 2015 Oct;169(10):929-937.
Image credit: Nationwide Children’s
About the author

Cody Hostutler, PhD, is a pediatric primary care psychologist at Nationwide Children’s Hospital and assistant professor in the Department of Pediatrics at The Ohio State University. He received training in integrated primary care at Lehigh University, The Children’s Hospital of Philadelphia, Nemours/A.I. DuPont Hospital for Children, and Geisinger Health System. His research interests include evaluating the effect that integrated primary care has on the quadruple aim (i.e., patient and provider satisfaction, clinical outcomes, reducing healthcare costs) as well as identifying and reducing health disparities.


