
A Surprising Approach to Classic Bladder Exstrophy
A Surprising Approach to Classic Bladder Exstrophy https://pediatricsnationwide.org/wp-content/uploads/2021/04/Surgical-Close-Up-1024x754.jpg 1024 754 Jeb Phillips https://pediatricsnationwide.org/wp-content/uploads/2021/03/Jeb-Phillips.jpg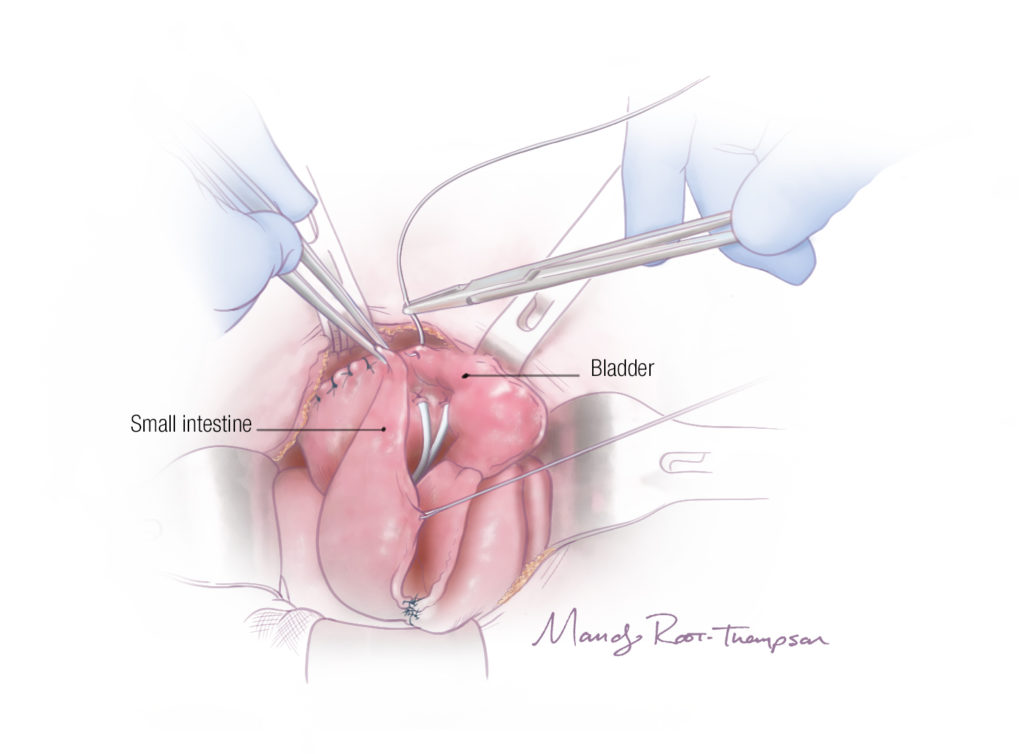
A procedure developed at Nationwide Children’s Hospital comes with possible risks but can have a huge impact on quality of life.
It’s become clearer over the last two years that a “good outcome” for children born with classic bladder exstrophy is in the eye of the beholder.
One of the best outcomes, nearly everyone would agree, is that a child with this complex congenital defect — often requiring multiple procedures over the course of years — would ultimately be able to urinate like a “normal” child. In fact, that is the question parents most often ask after a diagnosis, says V. Rama Jayanthi, MD, chief of Urology at Nationwide Children’s Hospital: “Will my child be normal?”
For decades, surgeons believed that many children could have that outcome. There were certainly individual examples of it. But the condition is relatively rare, and a patient’s potential procedures so spread out over time, so it was tough to track long-term outcomes.
Then, in late 2019 and early 2020, came the two largest studies ever published on bladder exstrophy outcomes — one from Nationwide Children’s and its peers in the Pediatric Urology Midwest Alliance, and another from Johns Hopkins Medical Institutions. They brought the bad news that experienced pediatric urologists had begun to suspect: true continence with normal urination was unusual, and only then with many major surgeries.
The outcome that most patients could expect was “staying dry” through clean intermittent catheterization every few hours for the rest of their lives, the studies found. From a medical perspective, that may well be considered a success, says Dr. Jayanthi.
“You have to consider quality of life as an outcome too,” he says. “The quality of life for a child who must catheterize every three hours, the quality of life for that child’s family, can be difficult. Many children are unhappy needing to catheterize. Is there a way we can address that?”
Dr. Jayanthi at Nationwide Children’s, and perhaps a handful of other pediatric urologists in the United States, believe there is one. The procedure is unusual enough that it doesn’t have a formal name, and Dr. Jayanthi himself admits many of his peers wouldn’t consider doing it.
In the right circumstances, though, and for certain children, it has been life changing.
“You have to absolutely lay it on the line with the families, tell them all the information you know, and then it has to be their choice. But that’s the point. Now there is a choice that they didn’t have before.”
– V. Rama Jayanthi, MD
TRADITIONAL APPROACHES TO EXSTROPHY
Bladder exstrophy is most obviously characterized by a malformed bladder protruding through the abdomen and exposed outside of the body. The urinary sphincter doesn’t work or doesn’t exist, so urine continually leaks, and often the urethra doesn’t exist either. Other body systems, especially the reproductive system, can be affected.
Many children born with the condition undergo an initial procedure at a few months of age to enclose the bladder inside the body. Reconstruction of the urethra and/or the penis may occur as well (the condition is about twice as prevalent in males as females).
Then, typically when a child would begin preschool or kindergarten, come complicated procedures intended to make a child continent. The bladder neck is tightened in an attempt at developing some urine control. However, as the large studies showed, the majority of bladder neck procedures in exstrophy cases don’t actually have that result. Incontinence continues and regular urination isn’t possible.
At that point, a child’s bladder neck may need to be closed or retightened, the bladder may need to be enlarged by adding intestinal tissue, and urine permanently diverted for the child to stay dry. The most common current approach creates a channel from the bladder through the abdomen using the appendix (called a Mitrofanoff procedure). The child is able to catheterize through the channel to remove urine. This method works and works well.
That’s a successful outcome with a potentially challenging quality of life for children who otherwise have no health issues.
The Division of Urology at Nationwide Children’s has spent the last decade more closely tying “successful outcome” with “quality of life.” Dr. Jayanthi began thinking about a new bladder exstrophy approach after he saw a patient who, in contrast to similar patients, had a relatively easy time voiding urine. The child had been adopted from Asia and treated there with a procedure largely abandoned in the United States called ureterosigmoidostomy. With that approach, ureters are detached from the bladder and attached to the sigmoid colon; urine bypasses the bladder entirely and exits the body through the rectum.
The child needs to go to the bathroom somewhat more often than other children, but no catheter is needed.
“She was just so much happier, and her family was so much happier, than other patients I have,” said Dr. Jayanthi. “She was a competitive gymnast growing up, and her bladder exstrophy diagnosis had little impact on her day-to-day life. I started thinking, can we do this here without the risks that usually come with it?”
The risks are why ureterosigmoidostomy had been abandoned. The connection of the ureters with the high-pressure system of the sigmoid colon can lead to feces reflux into the ureters, causing infection. More catastrophically, the incidence of colon cancer was shown to be many times greater than in the general population, presumably driven by the intermixing of feces and urine in the colon.
Dr. Jayanthi had a new take on this old idea that even his bladder exstrophy partner at Nationwide Children’s calls “shocking.”
“I knew Dr. Jayanthi had done a handful of these when I joined Nationwide Children’s as a fellow, and I honestly found it shocking. Rectal diversion would be considered only a salvage procedure by most people because of the risks of cancer. This fear is why we’re taught not to do it. That being said, for a family that fully understands the risks, this can result in a great quality of life.”
— Molly Fuchs, MD
A NEW WAY
With this new approach, urine still leaves the body through the rectum as it would in ureterosigmoidostomy, but the ureters stay connected to the bladder. The bladder is augmented, serves as a low-pressure reservoir and is connected to the rectum (instead of the colon) via a new channel. Urine flows from the reconstructed bladder to the rectum and leaves the body that way with no catherization. The rectal sphincter maintains continence. (For a detailed illustration of these procedures, see In Sight: A New Kind of Rectal Diversion in Classic Bladder Exstrophy.)
There is little chance for feces reflux into the ureters because they remain connected to the bladder, not attached to the colon or the rectum. Most of the urine is held in the bladder instead of the colon or rectum, so mixing with feces is reduced. Conceptually, infections should be less likely, and the patients who have had this procedure have experienced very few, says Dr. Jayanthi.
The risk of cancer may be reduced as well.
But there’s no way to know that yet, says Molly Fuchs, MD, a urologist at Nationwide Children’s who works with Dr. Jayanthi on exstrophy cases. That lack of evidence would give anyone pause, she says, and causes most urologists to avoid any sort of rectal diversion approach.
“I knew Dr. Jayanthi had done a handful of these when I joined Nationwide Children’s as a fellow, and I honestly found it shocking,” she says. “Rectal diversion would be considered only a salvage procedure by most people because of the risks of cancer. This fear is why we are taught not to do it. That being said, for a family that fully understands the risks, though, this can result in a great quality of life.”
Another pediatric urologist in the United States who has performed a version of a rectal diversion surgery is Patricio Gargollo, MD, of the Mayo Clinic. Dr. Gargollo was the senior author of the large exstrophy study published in late 2019 by the Pediatric Urology Midwest Alliance (Dr. Fuchs was a co-author). The group includes Nationwide Children’s, Mayo, Lurie Children’s Hospital, Cincinnati Children’s Medical Center, and Riley Hospital for Children, and was formed
by the five large institutions in part to share expertise on extremely rare conditions such as bladder exstrophy.
“Each child with bladder exstrophy is different, and every family has an individual perspective on it,” says Dr. Gargollo. “Rectal diversion is not going to be the best approach for many families. What our study helped show, though, is that what most urologists are doing now may not be the best approach for some families either. This is another option.”
Dr. Jayanthi, Dr. Gargollo and Dr. Fuchs all stress this.
Most families may still be best served by the procedures that result in regular catheterization. Nationwide Children’s and Mayo have used it and will continue to use it in the future. A family who is presented with the rectal diversion option must have a clear understanding of the possible benefits and future risks.
Honest conversations about classic bladder exstrophy and its outcomes are more possible now than they have ever been, thanks to the studies of the last two years.
For Dr. Jayanthi, those studies show a new approach is warranted.
“You have to absolutely lay it on the line with the families, tell them all the information you know, and then it has to be their choice,” he says. “But that’s the point. Now there is a choice that they didn’t have before.”
This article appeared in the Spring/Summer 2021 print issue. Download the full issue.
References:
- Szymanski KM, Fuchs M, Mcleod D, Rosoklija I, Strine AC, VanderBrink B, Whittam B, Yerkes E,
Gargollo PC; Pediatric Urology Midwest Alliance (PUMA). Probability of bladder augmentation, diversion and clean intermittent catheterization in classic bladder exstrophy: a 36-year, multi-institutional, retrospective cohort study. Journal of Urology. 2019 Dec;202(6):1256-1262. - Maruf M, Manyevitch R, Michaud J, Jayman J, Kasprenski M, Zaman MH, Benz K, Eldridge M, Trock B, Harris KT, Wu WJ, Di Carlo HN, Gearhart JP. Urinary continence outcomes in classic bladder exstrophy: a long-term perspective. Journal of Urology. 2020 Jan;203(1):200-205.
- Gargollo PC, Jayanthi R. Great expectations: the dream versus the reality of urinary continence and bladder exstrophy. Journal of Urology. 2020 Jan;203(1):46-47.
Image credit: Nationwide Children’s
About the author

Jeb is the Managing Editor, Executive Communications, in the Department of Marketing and Public Relations at Nationwide Children's Hospital. He contributes feature stories and research news to PediatricsOnline, the hospital’s electronic newsletter for physicians and other health care providers, and to Pediatrics Nationwide. He has served as a communications specialist at the Center for Injury Research and Policy at The Research Institute and came to Nationwide Children’s after 14-year career as daily newspaper reporter, most recently at The Columbus Dispatch.
- Jeb Phillipshttps://pediatricsnationwide.org/author/jeb-phillips/

- Jeb Phillipshttps://pediatricsnationwide.org/author/jeb-phillips/
- Jeb Phillipshttps://pediatricsnationwide.org/author/jeb-phillips/
- Jeb Phillipshttps://pediatricsnationwide.org/author/jeb-phillips/