
Paying for Telehealth After COVID-19
Paying for Telehealth After COVID-19 https://pediatricsnationwide.org/wp-content/uploads/2021/02/More-to-Telehealth_Page-28-1024x535.jpg 1024 535 Jeb Phillips https://pediatricsnationwide.org/wp-content/uploads/2021/03/Jeb-Phillips.jpg
Telehealth has become an essential part of health care delivery during the COVID-19 pandemic, but its future depends on reimbursement and other financial questions.
Just weeks into the COVID-19 pandemic in the United States, health care stakeholders across the country were talking about the expansion of telehealth as a silver lining, and how it seemed likely that a new era in care delivery was beginning.
“I think the genie’s out of the bottle on this one,” said Seema Verma, the administrator of the Centers for Medicare and Medicaid Services (CMS), in a widely shared April 2020 Wall Street Journal article. “I think it’s fair to say that the advent of telehealth has been just completely accelerated, that it’s taken this crisis to push us to a new frontier, but there’s absolutely no going back.”
A rush of federal and state action made that possible – initially, at least. Much of that action focused on who can be paid for telehealth services, which services they can be paid for, and how much they will be paid for delivering those services. The future of telehealth once the COVID-19 emergency is over will depend, in part, on the permanent answers to those financial questions, say people working on the issue.
Since telehealth became a viable way of delivering care in the last decade, Medicare policies have not kept pace, says Aimee Ossman, Vice President of Policy Analysis for Children Hospital Association. States have great flexibility on how to administer their individual Medicaid programs – which, in combination with the Children’s Health Insurance Program, are the largest insurers of children in the United States — but Medicare policies can set the tone for Medicaid and private insurance policies on telehealth.
There were concerns about patient privacy, security, fraud and quality of care. But there was also the belief that telehealth would be expensive.
“The Congressional Budget Office has said telehealth has a high price tag, because they don’t see telehealth as replacing in-person visits,” Ossman says. “They see it as an addition. COVID is giving us an opportunity to collect data to refute this.”
In an effort to address the pandemic, Congress allowed the U.S. Department of Health and Human Services to relax restrictions on Medicare telehealth in early March, and CMS encouraged states to allow more flexibility in Medicaid telehealth. According to a recent report from the national Taskforce on Telehealth Policy, every state took some emergency action, such as easing licensure laws to facilitate care across state borders.
The majority of states also expanded the number of services that could be provided via telehealth, the kinds of providers who could offer services, and the originating locations of telehealth appointments (including at home). A total of 32 states also allowed for some telehealth services to be reimbursed at the same rates as in-person services.
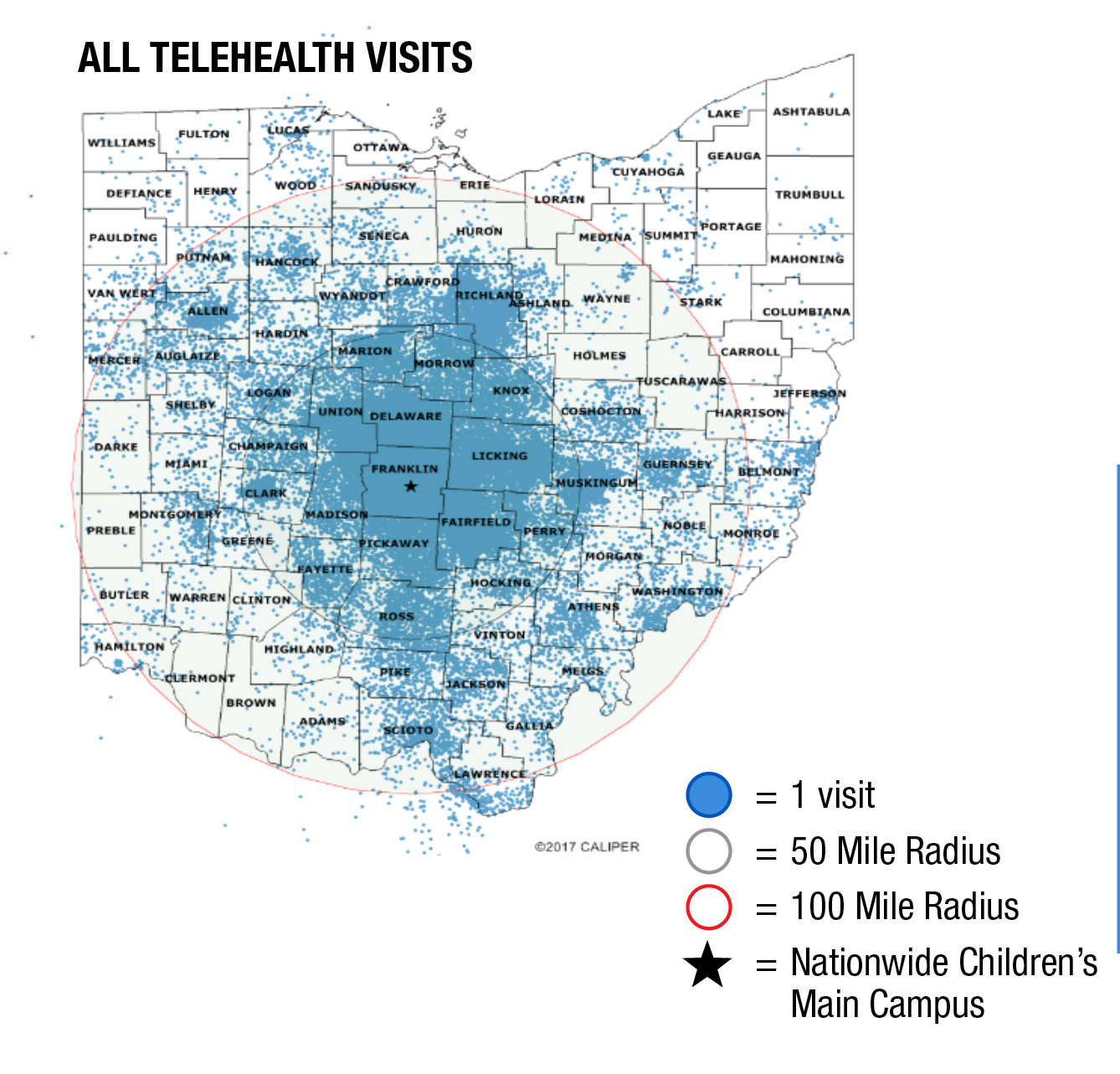
Ohio’s governor and Department of Medicaid quickly moved to relax emergency Medicaid rules in March and increase the services and providers who could be reimbursed. That helped Nationwide Children’s Hospital go from offering a smattering of telehealth appointments in all of 2019 to as many as 2,000 per day in April and May of 2020.
In early September, Ohio Medicaid director Maureen Corcoran began the process of making those emergency rules permanent. Nationwide Children’s and Ohio’s other children’s hospitals had been advocating for this, and it will benefit the state’s children and families, says Charlie Solley, Nationwide Children’s vice president of Government Affairs.
“The issue across the country, though, is that if you’ve seen one state Medicaid program . . . you’ve seen one state Medicaid program. Each one is different from the other, and they have different ways of operating,” says Solley. “Just because we have seen telehealth success in Ohio, and Ohio’s governmental leaders want to build on that success, doesn’t mean that other states will do the same.”
In the Medicaid and child health realms, most of the advocacy efforts are happening at the state level for that very reason, says Ossman of the Children’s Hospital Association. Congress and CMS have the ability to make federal Medicare rules permanent, encourage that states to do the same for Medicaid and mandate coverages for commercial insurers, but federal policymaking outside of an emergency is often a slow process, she says.
What may encourage the ongoing availability and reimbursement of telehealth are the data regarding cost and outcomes that are being collected during the pandemic. The national Taskforce on Telehealth Policy found that in most cases it studied, telehealth was used as a substitute for in-person care, not in addition to it, allaying some concern about increased charges.
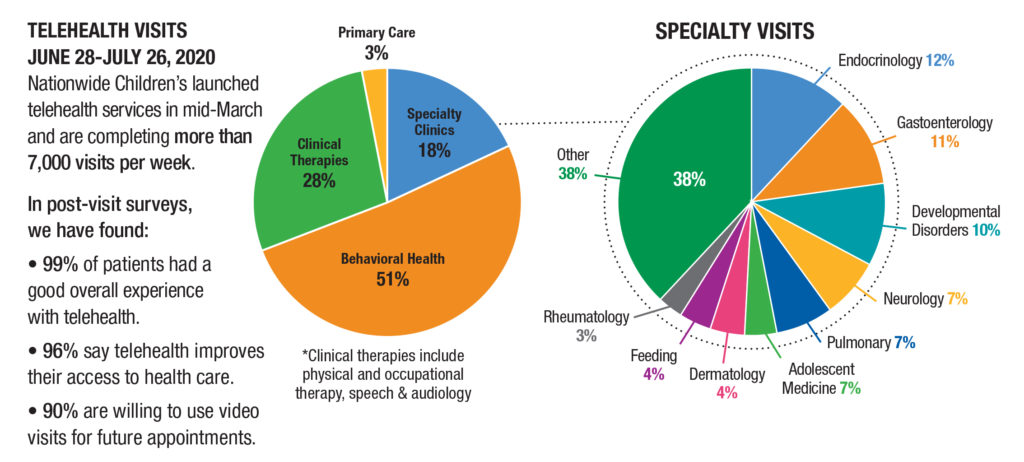
The notable exception to that finding was in behavioral health, where there has been an overall increase in utilization – more people are using behavioral health services now than before the pandemic. Taskforce members hypothesized that is the result of stress brought on by COVID-19, the removal of regulatory barriers, the lessened stigma of receiving behavioral health care at home through telehealth, or some combination of all of those. Many observers have long felt that behavioral health is particularly well-suited to telehealth technology, and Eric Butter, PhD, chief of Pediatric Psychology & Neuropsychology at Nationwide Children’s, estimates that 92% of the hospital’s patients can have an effective psychological evaluation via telehealth.
Beyond direct health care cost data, Nationwide Children’s has found that the families it serves have experienced a number of savings as a result of telehealth expansion, including thousands of fewer days taken off work and tens of thousands of fewer hours spent traveling. In post-visit surveys, 96% of families said telehealth improves their access to care.
Beyond the emergency use case during COVID-19, there are lots of reasons to be optimistic about the future of telehealth, says Hilary Daniel, Manager, Policy Analysis at Children’s Hospital Association. There’s bipartisan support for it and building evidence that families have benefitted. Money, however, may be a sticking point for a long time to come.
“A few common themes show up in the discussion of telehealth, and reimbursement might be the biggest one,” she says. “Providers want it to be consistent and appropriate. They want a balance between telehealth and in-person reimbursement. We know that reimbursement is driving adoption of telehealth for providers across the country, and it will be some time before we know how the issue will be resolved.”
References:
- Editorial Board. The doctor will Zoom you now. Wall Street Journal. April 26, 2020. Accessed Sept. 25, 2020. https://www.wsj.com/articles/the-doctor-will-zoom-you-now-11587935588
- Taskforce on Telehealth Policy. Taskforce on Telehealth Policy Findings and Recommendations. September 2020. Accessed Sept. 25, 2020. https://www.ncqa.org/programs/data-and-information-technology/telehealth/taskforce-on-telehealth-policy/taskforce-on-telehealth-policy-ttp-findings-and-recommendations/
Image credits: Nationwide Children’s
About the author

Jeb is the Managing Editor, Executive Communications, in the Department of Marketing and Public Relations at Nationwide Children's Hospital. He contributes feature stories and research news to PediatricsOnline, the hospital’s electronic newsletter for physicians and other health care providers, and to Pediatrics Nationwide. He has served as a communications specialist at the Center for Injury Research and Policy at The Research Institute and came to Nationwide Children’s after 14-year career as daily newspaper reporter, most recently at The Columbus Dispatch.
- Jeb Phillipshttps://pediatricsnationwide.org/author/jeb-phillips/

- Jeb Phillipshttps://pediatricsnationwide.org/author/jeb-phillips/
- Jeb Phillipshttps://pediatricsnationwide.org/author/jeb-phillips/
- Jeb Phillipshttps://pediatricsnationwide.org/author/jeb-phillips/

