
Opening the Door to Adult Medicine
Opening the Door to Adult Medicine https://pediatricsnationwide.org/wp-content/uploads/2019/05/062615ds3218_header-1024x575.jpg 1024 575 Katie Brind'Amour, PhD, MS, CHES https://pediatricsnationwide.org/wp-content/uploads/2021/03/Katie-B-portrait.gif
Care transition plans aren’t just for kids with congenital conditions anymore. Could your practice benefit from a proactive transition plan for all patients?
In the shift from pediatric to adult care, young patients have the responsibility to adjust to a new life of self-management. But health care providers also play an important role in this rite of passage.
Some physicians believe that care transition planning is both important and practical to implement for children of all health statuses. Others believe it is most reasonable to leave care transition planning to pediatric subspecialists – those in charge of the most complicated care for the most complex patients with chronic conditions.
Which approach is most feasible and appropriate? And how can physicians who are new to the practice begin to implement transition planning?
COMING TO TERMS WITH THE CONCEPT
The definition of care transition varies both by patient population and provider, but it typically encompasses the migration of young adults from the pediatric health care world into the realm of adult medicine, with personal health obligations shifting to the patient. And in all cases, care transition is more than a simple referral.
“The majority of patients seen by a generalist are going to be a ‘referral plus’ – kids who don’t have a lot of health problems who are leaving high school, with limited health concerns in the background that need to be made known to an adult practitioner who will take them over,” says Karen McCoy, MD, chief of the Section of Pulmonary Medicine at Nationwide Children’s Hospital.
For generally healthy children, she says, transitioning mostly involves sending the medical records and doing a quick call or letter if needed to explain important health history or management needs, plus having a chat with the patient and family to discuss who they’re being referred to and whether they have any questions.
“Preparing to transition a patient with a highly specialized condition and lots of comorbidities is obviously more of an ordeal,” says Dr. McCoy, who has developed and implemented a detailed care transition program involving face-to-face education for patients who have cystic fibrosis and other pulmonary conditions. A paper detailing her team’s highly protocolized efforts is pending publication. “It’s important to start prepping them no later than the mid-teens about the need to transition and to develop skills to manage their own care once they are an adult.”
For patients with congenital issues requiring lifelong care, preparation may begin even earlier, with many groups at Nationwide Children’s initiating the topic at age 12 or younger.
No matter the complexity of care needs, however, care transition involves the segue from being treated as a child to being treated as an adult – both in the parental sense and medical sense. Responsibility will eventually fall on the young patient to know when to fill prescriptions, how to take medications, what to put in an advanced health care directive, how to monitor symptoms and when to reach out to a pharmacist or physician. This self-sufficiency certainly isn’t learned overnight.
“From day one, we raise the topic that eventually they will be transitioned to an adult care provider, just to set that expectation. We then periodically revisit that talk as patients get closer to adolescence, and around age 12, we start doing transition readiness surveys for patients and parents,” says Alessandra Gasior, DO, director of Colorectal Transition of Care at the Center for Colorectal and Pelvic Reconstruction at Nationwide Children’s. The program is the first to connect Nationwide Children’s patients with irritable bowel disease, Hirschsprung disease and anorectal malformations to adult providers at The Ohio State University Wexner Medical Center. “For someone with a congenital or lifelong problem who has been coming to a pediatric center their entire life, it can take a lot of time and effort to create a smooth transition for the patient – you need everyone to be familiar with each other and the specific care required.”
CHALLENGES TO EFFECTIVE TRANSITIONS
The concept of handing over care is fairly straightforward, but its historic implementation has been inconsistent and often ineffective at best. Research continues to uncover the loss to follow-up and poor health outcomes experienced by young adults with various health conditions who fail to transition effectively. Patients who discontinue needed care often present years later with severe or urgent health problems that could have been avoided with proper ongoing management. On the flipside, patients who experience planned and facilitated hand-offs to adult practitioners tend to fair better than those with no assistance.
The barrier to facilitating an effective transition is more nuanced than a simple lack of time or effort on behalf of patients or physicians, however. Especially among patients who have long received care from a pediatric practice, the importance of a supportive and welcoming environment in their next care experience may override the basic understanding that health services are critical for their wellbeing.
“If patients can establish a good relationship with the new provider, they will go back for care,” says Dr. Gasior. “But the difference in adult and pediatric centers can be shocking for patients – they’re alone and have to be independent and autonomous, and people treat them differently.”
This problem may be particularly pertinent for the many freestanding children’s hospitals with limited physical or referral ties to adult institutions. Although separation has allowed great growth in pediatric hospital size and expertise, it has also created the hurdle of changing locations and health systems.
The jarring difference is compounded by the problem of having few adult practitioners available who understand certain congenital or historically pediatric diseases. Some physicians struggle to locate an adult care provider who is willing and able to take on the long-term management of a patient with these conditions, such as congenital heart disease, myelomeningocele and cystic fibrosis. The disparity in knowledge is a two-way street, however.
“Most patients with lifelong pediatric conditions seem to prefer staying at their pediatric centers, and if we could provide that specialized care it would be ideal,” says Daniel DaJusta, MD, medical director of the Center for Colorectal and Pelvic Reconstruction in the Section of Urology at Nationwide Children’s. “But when they get to a certain age they start to have real adult problems that have nothing to do with what we do in pediatrics, and at that point they need adult providers like everyone else. Adult care is better provided in an adult hospital.”
The Section of Urology currently continues to see patients with complex congenital problems into adulthood due to a lack of adult providers familiar with congenital urologic conditions, but a formal transition collaboration with urologists at The Ohio State University Wexner Medical Center is under development.
“The disconnect between what we take care of in pediatric subspecialties and adult medicine – not just in age but life stages, and structural differences due to congenital versus acquired conditions – is at the crux of why care transition matters,” says May Ling Mah, MD, director of ACHD In-Patient Services in The Heart Center at Nationwide Children’s and a practitioner in Nationwide Children’s Adolescent and Adult Congenital Heart Disease Program.
Dr. Mah believes a global adult transition program – one in which adult providers housed within freestanding children’s hospitals offer onsite care for adult-related problems as well as pediatric-specific health issues – may offer a creative way to address this growing challenge.
LOOKING AT LOGISTICS
The general consensus in care transition planning is that something is probably better than nothing. But the devil is always in the details.
“All kids need a transition process. It’s really just developmental and learning how to navigate the health system when they become young adults,” says Stacy Ardoin, MD, section chief of Rheumatology at Nationwide Children’s, an active contributor to the development of condition-specific transition guidelines for the American College of Rheumatology, and a clinician-researcher engaged in numerous studies on the transition process. “But not every person, chronic disease or not, needs the same level of intense support. We need a way to identify those individuals at risk for not having a good transition and then tailor more intense support for them.”
For this reason, readiness assessment is key. When resources are limited (and perhaps even when they’re not), those who would suffer the most from a disconnect in care or who are least likely to be able to transition independently should be the focus of physicians’ attention in the provision of active care transition planning.
In practice, care transition planning can be initiated with little effort. For example, physicians can simply begin asking patients between the ages of 12 and 16 about their understanding of their own care and future responsibilities. Physicians can then gradually work toward appointments wherein primarily the child answers the questions and discusses their care needs, rather than the parent.
“We do know that patients who have gone through an orderly transition process are more likely to show up at their adult provider and have other markers of compliance with medications,” says John Mahan, MD, program director for the Pediatric Residency Program for Nationwide Children’s and The Ohio State University. “It would be nice to see more outcomes data on care transitions so we can see which approaches are the best. Until we know that, however, it’s important to simply recognize the importance of having a system – an intentional process for assessing transition readiness and teaching kids to take on their own management.”
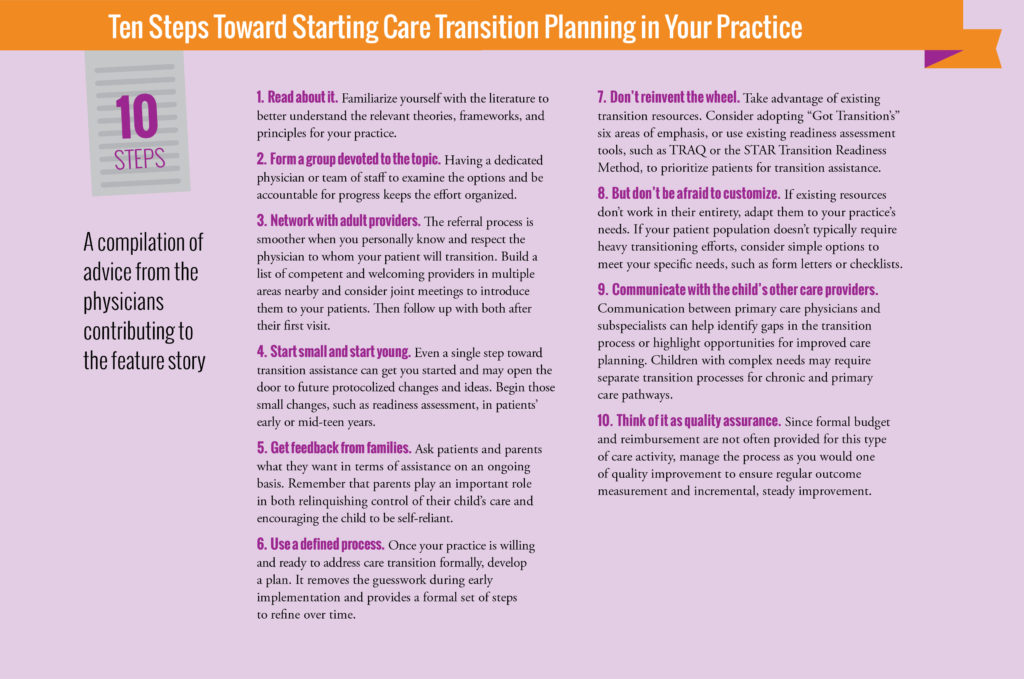
For those practices – subspecialty or otherwise – that want ready-made tools and guides to incorporate into a formal plan, options abound. A popular resource for existing toolkits and foundational materials is GotTransition.org, which offers a collection of practice resources for children with a wide range of chronic conditions as well as some general readiness assessment tools and customization strategies.
Other options exist as well, including the Transition Readiness Assessment Questionnaire (TRAQ) and the University of North Carolina STAR Transition Readiness Method, both highlighted in context with numerous other strategies for implementing care transition efforts in an article on the topic authored by Dr. Mahan last year in Pediatrics in Review. The academic literature is flooded with other tools for myriad conditions as well as advice for primary care.
Essentially, the distinction between a basic referral and effective care transition hinges on physician involvement, readiness assessment and proactive, organized preparation. Guiding all children – and their parents – toward more independent care and active adulthood participation in essential health-related self-care is a lofty goal, but it is a goal that may one day be expected as standard care for patients of all health care needs.
About the author

Katherine (Katie) Brind’Amour is a freelance medical and health science writer based in Pennsylvania. She has written about nearly every therapeutic area for patients, doctors and the general public. Dr. Brind’Amour specializes in health literacy and patient education. She completed her BS and MS degrees in Biology at Arizona State University and her PhD in Health Services Management and Policy at The Ohio State University. She is a Certified Health Education Specialist and is interested in health promotion via health programs and the communication of medical information.
- Katie Brind'Amour, PhD, MS, CHEShttps://pediatricsnationwide.org/author/katie-brindamour-phd-ms-ches/

- Katie Brind'Amour, PhD, MS, CHEShttps://pediatricsnationwide.org/author/katie-brindamour-phd-ms-ches/
- Katie Brind'Amour, PhD, MS, CHEShttps://pediatricsnationwide.org/author/katie-brindamour-phd-ms-ches/
- Katie Brind'Amour, PhD, MS, CHEShttps://pediatricsnationwide.org/author/katie-brindamour-phd-ms-ches/


