Technical Aspects of Fetal Aortic Valvuloplasty Predict Success of the Procedure
Technical Aspects of Fetal Aortic Valvuloplasty Predict Success of the Procedure https://pediatricsnationwide.org/wp-content/uploads/2019/04/Insight-Left-Side_FINAL-for-web-header-1024x575.jpg 1024 575 Mary Bates, PhD https://secure.gravatar.com/avatar/d8c01b42dd4f98ebe33b59a37151ffdb0226803d9094f30793729669defbdf99?s=96&d=mm&r=g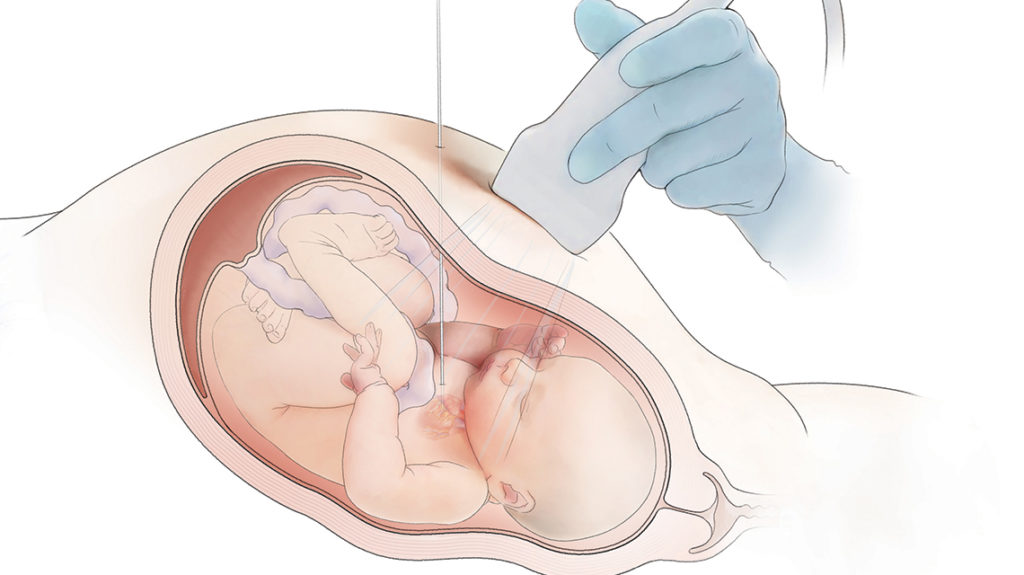
The procedure is often successful but comes with significant risks to fetal health and life.
Fetal aortic valvuloplasty (FAV) is a procedure performed mid-gestation in a subset of fetuses with aortic stenosis who would likely develop hypoplastic left heart syndrome with no intervention. Although often successful, it is a high-risk procedure that is associated with significant rates of complications and fetal mortality.
In a recent study, researchers from institutions including Nationwide Children’s Hospital evaluated how technical aspects of FAV impacted procedural risks and pregnancy outcomes. The researchers gathered data from the International Fetal Cardiac Intervention Registry on fetuses who underwent the procedure from 2002 to 2018.
“We found that technical success was the strongest predictor of live birth,” says Aimee Armstrong, MD, director of Cardiac Catheterization & Interventional Therapies at Nationwide Children’s and one of the study’s authors.
“Success is really dependent on getting the proper trajectory. You need that needle to come in the apex of the left ventricle and be pointed right at the aortic valve.”
Mortality within the first 48 hours was 16.7%, relatively higher than what has been reported in other studies. This may be due to the heterogeneity of the centers involved, which may have differing amounts of experience or vary in their procedural technique.
Dr. Armstrong and her colleagues found that complications were prevalent, occurring in nearly half of all attempted interventions. Multiple cardiac punctures were associated with increased rates of complications and fetal mortality and lower rates of technical success.
The researchers also found that larger needle size was associated with higher rates of pericardial effusion, a complication that can lead to fetal demise.
“We learned that we want to use as small a catheter as possible,” says Dr. Armstrong, who is also a professor of Pediatrics at The Ohio State University College of Medicine. “But some people choose larger needles because they want to use a larger balloon for improved opening of the aortic valve. That’s one thing we need to weigh when figuring out what size needle to use.”
Dr. Armstrong says the study shows that clinicians should use as small a needle as they can for the balloon size they think will be effective.
“Plus, if we aren’t successful on the first cardiac puncture, we need to really weigh the risks and benefits of a second cardiac puncture because with each puncture, the chances of success go down and the complications go up,” she says.
Dr. Armstrong and her colleagues still want to know if FAV is decreasing morbidity and mortality in the long-term. She notes a trial in Europe that is prospectively following patients who do and do not undergo the procedure and says these data will tell us more than querying the registry.
“Studies like those will help us determine if this is the right thing to do for a fetus at 23 weeks gestation,” she says. “We think it is, right now, if we’re seeing hypoplastic left heart syndrome evolving. The problem is, we don’t know for sure that it’s the right thing to do.”
Reference:
Patel ND, Nageotte S, Ing FF, Armstrong AK, Chmait R, Detterich JA, Galindo A, Gardiner H, Grineco S, Herberg U, Jaeggi E, Morris SA, Oepkes D, Simpson JM, Moon-Grady A, and Pruetz JD. Procedural, pregnancy, and short-term outcomes after fetal aortic valvuloplasty [published online ahead of print, 2020 Mar 26]. Catheter Cardiovasc Interv. 2020;10.1002/ccd.28846. doi:10.1002/ccd.28846.
Image Credit: Nationwide Children’s
About the author
Mary a freelance science writer and blogger based in Boston. Her favorite topics include biology, psychology, neuroscience, ecology, and animal behavior. She has a BA in Biology-Psychology with a minor in English from Skidmore College in Saratoga Springs, NY, and a PhD from Brown University, where she researched bat echolocation and bullfrog chorusing.
- Mary Bates, PhDhttps://pediatricsnationwide.org/author/mary-bates-phd/

- Mary Bates, PhDhttps://pediatricsnationwide.org/author/mary-bates-phd/
- Mary Bates, PhDhttps://pediatricsnationwide.org/author/mary-bates-phd/
- Mary Bates, PhDhttps://pediatricsnationwide.org/author/mary-bates-phd/