
How Can We Make Child Health Equitable?
How Can We Make Child Health Equitable? https://pediatricsnationwide.org/wp-content/uploads/2021/04/Health-Equity-1.jpg 550 350 Jeb Phillips, Abbie Miller and Natalie Wilson https://pediatricsnationwide.org/wp-content/uploads/2021/03/Jeb-Phillips.jpg
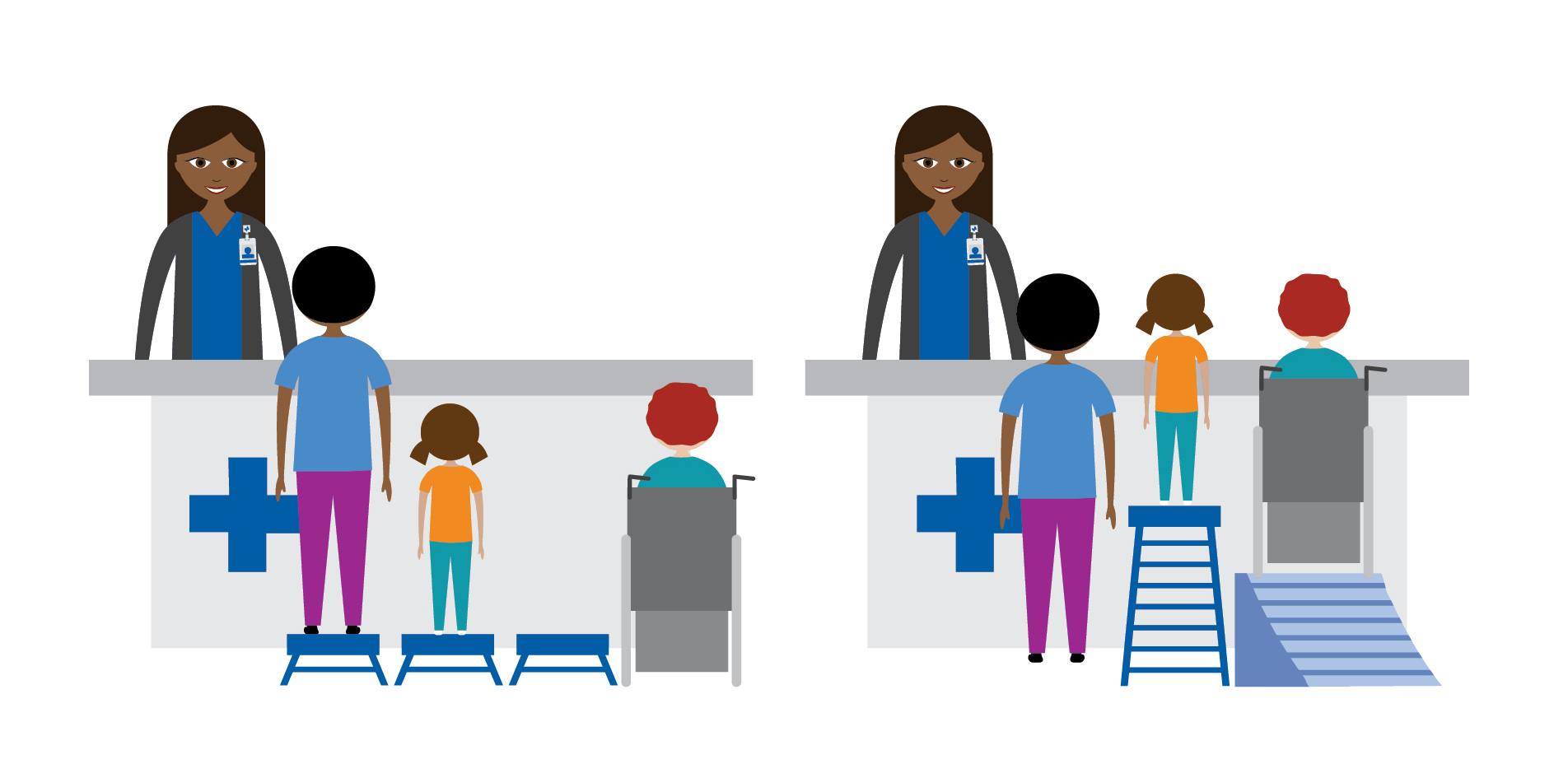
Researchers in the Center for Child Health Equity and Outcomes Research at Nationwide Children’s Hospital are tackling this question by identifying health disparities and uncovering exactly how social drivers of health impact outcomes.
“Health equity means that everyone has a fair and just opportunity to be as healthy as possible.”
That’s how the Robert Wood Johnson Foundation, the largest health-focused philanthropic organization in the United States, defines the concept of health equity.
The widely recognized definition goes on to say that achieving health equity “requires removing obstacles to health such as poverty, discrimination, and their consequences, including powerlessness and lack of access to good jobs with fair pay, quality education and housing, safe environments and health care. For the purposes of measurement, health equity means reducing and ultimately eliminating disparities in health and its determinants that adversely affect excluded or marginalized groups.”
Income, education, employment and systemic bias are all related to health and health outcomes. These social drivers of health are the subject of a growing body of research that is dedicated to understanding underlying causes of health disparities and inequities experienced by racial/ethnic, sexual orientation and gender identity minorities.
Achieving health equity has long been a priority at Nationwide Children’s Hospital. Its founding mission in 1892 was that all children should receive care regardless of a family’s ability to pay, a statement of “health equity” before that term had been defined. In the decades since, strategic plans have been built around the idea that a “zip code should not determine a child’s health,” in the words of Steve Allen, MD, the hospital’s CEO emeritus.
Research throughout the Nationwide Children’s organization has guided those plans by revealing that social drivers of health affect health equity and access to care. Now, that work is forming the basis of the new Center for Child Health Equity and Outcomes Research at the Abigail Wexner Research Institute at Nationwide Children’s.
“Health disparities are not usually rooted in biology. They are created and supported by social constructs and systems that limit access to health care and upward mobility,” says Deena Chisolm, PhD, vice president of Health Services Research at Nationwide Children’s and director of the new center. “And barriers to health equity exist in all areas of clinical care, health services and communities.”
“Our mission in the Center for Child Health Equity and Outcomes Research is to address inequities and outcomes through research across all of these areas. We are here to support and be integrated with existing research and clinical programs across the Nationwide Children’s enterprise.”
 Health Equity and Anti-Racism
Health Equity and Anti-Racism
“You can’t talk about child health equity without acknowledging the impact of racism on the health of communities, families and children,” says Dr. Chisolm. “Structural racism, and the unconscious biases that accompany it, has created and enabled many of the biggest health disparities American children face.”
These biases can affect the quality of communication between providers and patients. A recent paper published by Dr. Chisolm and her team found that African American teens with chronic illnesses and their parents are less likely to report that their doctors spent enough time with them. According to Dr. Chisolm, whether this is the results of overtaxed providers in minority communities or unconscious biases, the end result is African American patients getting less of the support, education and counseling needed for good health management.
Understanding the Health Needs of Minority Populations
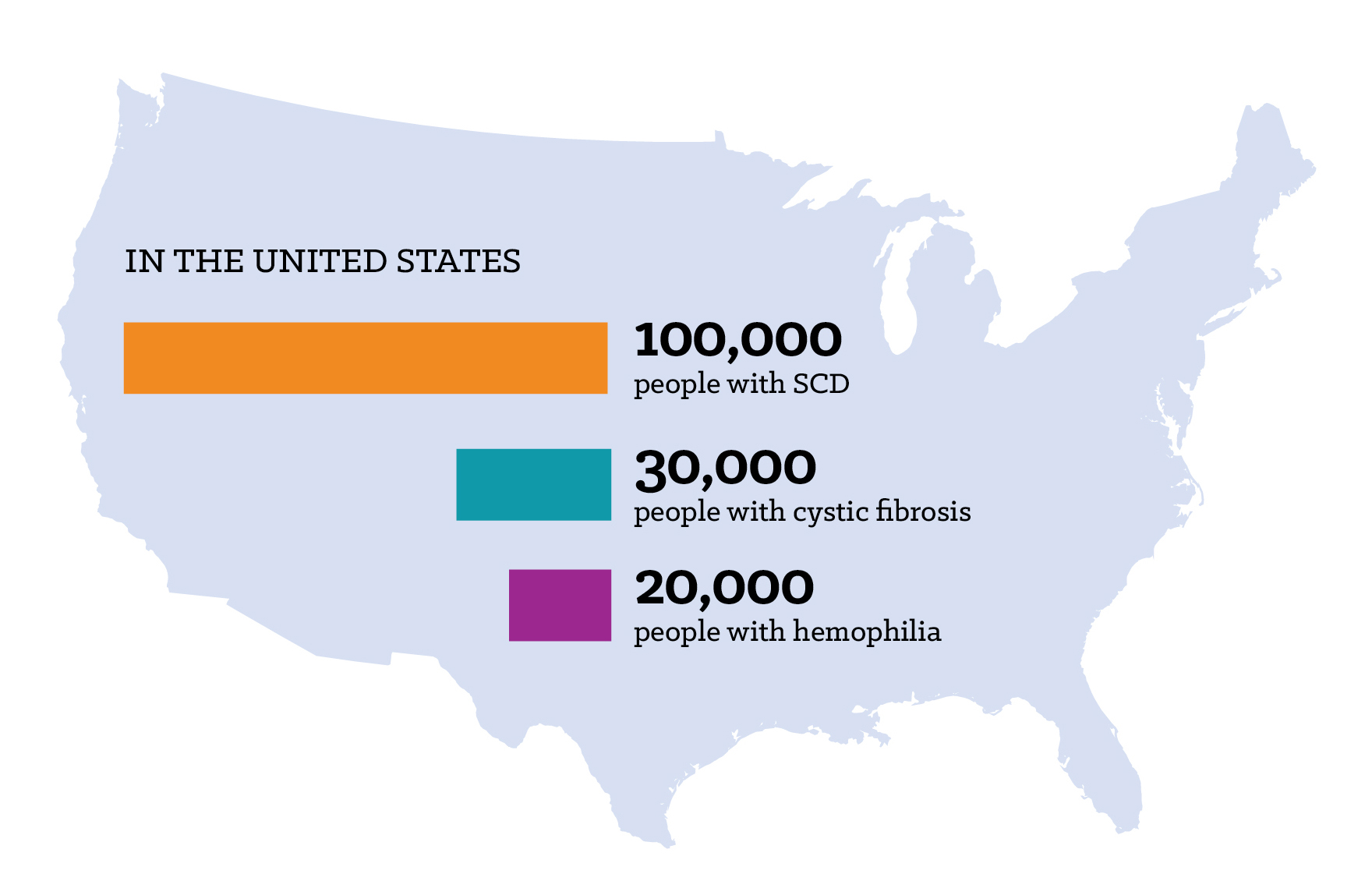
Medical conditions that are concentrated in minority populations, who already face many other disparities, have historically received less attention than other similar conditions. One such condition is sickle cell disease (SCD), which is more commonly diagnosed in African American children, and specifically SCD pain management.
Approximately 1 in 365 African Americans and 1 in 16,300 Hispanic Americans are born with SCD. And while SCD is three times more common than other genetic disorders in the United States, there are fewer treatment options and less public education about the disease. Studies have shown that SCD research receives less federal funding and foundation expenditures compared to these other disorders. Studies have also shown that black children are less likely to receive adequate pain control compared to white children.
“Severe pain is common in SCD, and few treatments other than opioids provide adequate SCD pain relief. While Ohio’s opioid guidelines were implemented to curb the opioid epidemic, their impact on children with SCD who require access to opioids to manage their pain had not been studied,” says Susan Creary, MD, hematologist and principal investigator in the center.
Dr. Creary and her colleagues had concerns about whether these guidelines could worsen pain management among patients who already faced the most challenges to adequate pain control. Results of their 2020 study, published in Pain Medicine, showed that Ohio’s 2013 and 2016 opioid prescribing guidelines to limit excessive opioid prescribing, filling and misuse were associated with significant but non-sustained changes to opioid prescription filling among children with SCD.
“Our findings showed that these guidelines resulted in only temporary changes in opioid filling among these children and may suggest that access to opioids among children with SCD at baseline is not excessive,” says Dr. Creary.
The Rural—Urban Divide
Access to care is a challenge that can be compounded by a range of factors, including transportation, number of providers available and, in the age of telehealth, internet access. And while children everywhere can experience barriers to accessing care, children living in rural areas often experience unique challenges.
“Some rural counties may not have any pediatricians — not to mention pediatric subspecialists,” says Kelly Kelleher, MD, MPH, vice president of Community Health at Nationwide Children’s and a principal investigator in the new center. “When we look at health equity for rural communities, we have to consider this.”
In a study published in Academic Pediatrics in 2020, Dr. Kelleher and his team investigated the contributions of social drivers of health to rural-urban preventive care differences among Medicaid enrollees. Among the more than 450,000 Medicaid enrollees in the study, just over 61% of urban children received a well-child visit. In large rural cities and small rural towns, 58% and 55.5% received well-child visits, respectively.
“In comparing small towns to urban centers, nearly 90% of the 5.7 percentage-point gap was explained by patient, parent and provider social drivers. The largest part of the rural-urban preventive care gap can be explained by differences in provider type, poverty, unemployment, and education levels,” says Dr. Kelleher. “We have more work to do in addressing these factors to improve pediatric preventive care in all communities.”
Institutions and organizations most involved in health equity issues are often located in metropolitan areas, and their initiatives often focus in those areas — either because of proximity or the expectation that more children can be impacted. Nationwide Children’s began a school-based asthma therapy program in Columbus City Schools, for example, improving access to preventive medications and ultimately reducing pediatric emergency department visits throughout Franklin county, where the school system is located. While the program has now expanded into many other districts, progress in rural counties has lagged.
In addition, health equity-focused organizations located in cities haven’t earned the trust of health care providers and consumers in rural counties.
“While we might have some ideas about what could work in rural counties, it is important that we not rush into those areas dictating changes, telling the providers there how to run things,” says Dr. Kelleher. “Particularly in Appalachian areas, communities may not broadly trust an outsider from an urban area who wants to come in and tell them how to do things.”
Furthermore, in many rural, particularly Appalachian counties, in Ohio, there simply isn’t the funding or workforce available to implement many of the guidelines or recommendations that come from large urban-based institutions.
“We need to build partnerships — the providers in these rural areas have a deep connection to the people they serve and a deep understanding of social drivers of health unique to the community that impact the people’s health there. They also know what resources are available and how to make those resources stretch,” says Dr. Kelleher. “Only by working together will we be able to move the needle on health outcomes in rural communities.”
Housing and Health Equity
A huge body of medical literature, dating from at least the 1980s, has examined the intersection of homelessness or housing instability and health. Health issues can lead to homelessness, and homelessness can lead to health issues. Homelessness and housing instability can also impact the way that people can seek care for their health issues. All of this is compounded for children, who have little say in where or how they live.
In fact, housing is sometimes considered the central social driver of health. It is difficult to be healthy without a stable home. Racism, poverty, job opportunities, neighborhood safety and a host of other factors influence housing, and housing has an influence on those factors as well. It’s why Nationwide Children’s has made housing a core focus of research and interventions.
In January, a study led by the Center for Child Health Equity and Outcomes Research showed for the first time that overall poor housing quality, not just homelessness and housing instability, is independently associated with poorer children’s health. Each housing quality issue, such as large holes in the floor or pest infestation, was linked to worse health status.
“Even when you adjust for demographic factors like race, ethnicity and disability, and housing-related issues like inability to pay rent or neighborhood safety, poor housing quality has an independent association with poorer health and higher health care use,” says Samantha Boch, PhD, RN, the lead author of the study, who completed it as a postdoctoral fellow at Nationwide Children’s. She is now an assistant professor at the University of Cincinnati College of Nursing and an affiliate faculty member of the James M. Anderson Center for Health Systems Excellence at Cincinnati Children’s Hospital Medical Center.
This kind of research has led Nationwide Children’s to make real-world changes in community housing. Its Healthy Neighborhoods Healthy Families initiative, founded in 2008, has now built or improved more than 400 homes and 115 rental units and drawn investments of more than $40 million to the historically disadvantaged South Side of Columbus. The initiative also coordinates workforce development, educational mentoring, tax preparation clinics and other programs.
That is not enough, however. Dr. Chisolm, Dr. Kelleher and others are conducting research around Healthy Neighborhoods Healthy Families to learn how the interventions are working. Some results will take decades to fully materialize, but there is some evidence of overall positive effect on high school graduation, health care utilization and neighborhood safety.
This article appeared in the 2021 Spring/Summer print issue. Download the full issue.
References:
- Creary SE, Chisolm DJ, Wrona SK, Cooper JN. Opioid prescription filling trends among children with sickle cell disease after the release of state-issued guidelines on pain management. Pain Medicine. 2020 Oct 1;21(10):2583-2592.
- Hardy RY, Liu GC, Kelleher K. Contribution of social determinant of health factors to rural-urban preventive care differences among Medicaid enrollees. Academic Pediatrics. 2021 Jan-Feb;21(1):93-100.
- Boch SJ, Taylor DM, Danielson ML, Chisolm DJ, Kelleher KJ. ‘Home is where the health is’: Housing quality and adult health outcomes in the Survey of Income and Program Participation. Preventive Medicine. 2020 Mar;132:105990.
- Chisolm DJ, Keedy HE, Dolce M, Chavez L, Abrams MA, Sanders L. Do health literacy disparities explain racial disparities in family-centered care for youths with special health care needs? Patient Education and Counseling. 2020 Sep 27. [ePub ahead of print]
Image credits: Nationwide Children’s
About the author

Jeb is the Managing Editor, Executive Communications, in the Department of Marketing and Public Relations at Nationwide Children's Hospital. He contributes feature stories and research news to PediatricsOnline, the hospital’s electronic newsletter for physicians and other health care providers, and to Pediatrics Nationwide. He has served as a communications specialist at the Center for Injury Research and Policy at The Research Institute and came to Nationwide Children’s after 14-year career as daily newspaper reporter, most recently at The Columbus Dispatch.

Abbie (Roth) Miller, MS, MWC, is a passionate communicator of science. As the manager of medical and science content at Nationwide Children’s Hospital, she shares stories about innovative research and discovery with audiences ranging from parents to preeminent researchers and leaders. She is a Medical Writer Certified®, credentialed by the American Medical Writers Association, and received her masters of science in Health Communication from Boston University.
Natalie is a passionate and enthusiastic writer working to highlight the groundbreaking research of the incredible faculty and staff across Nationwide Children's Hospital and the Abigail Wexner Research Institute. Her work at Nationwide Children's marries her past interests and experiences with her passion for helping children thrive and a long-held scientific curiosity that dates back to competing in the Jefferson Lab Science Bowl in middle school. Natalie holds a bachelor’s degree in sociology from Wake Forest University, as well as minors in women's, gender & sexuality studies and interdisciplinary writing. As an undergraduate student, Natalie studied writing and journalism, engaged with anthropological and sociological research with a focus on race and ethnic relations, served as executive editor for the student newspaper, the Old Gold & Black, and gained marketing experience as an intern for a nonprofit entrepreneurial incubator, Winston Starts, as well as by working for Wake Forest University School of Law Office of Communication and Public Relations and its Innocence and Justice Clinic.
-
Natalie Wilsonhttps://pediatricsnationwide.org/author/natalie-wilson/


